
Are CGMs Worth It?
Four weeks of glucose data will teach you more than any food chart. Whether you keep wearing it after that depends on what you need.


I’ve been wearing a continuous glucose monitor for five years. For the first month, the data was genuinely revelatory. Rice spikes me harder than ice cream. Wheat, not so much. A close friend that I went to elementary, middle and high school with, has the exact opposite pattern. That month changed how I eat.
4-6 weeks in, the CGM wasn’t telling me anything new. I developed a sense of how my body responded to every food I regularly eat. I kept wearing it past the 4-6 week, and it unexpectedly became an accountability tool.
TL;DR
The first 4-6 weeks of CGM data is genuinely revelatory. Individual glycemic responses vary by 5x for identical foods, and population nutrition charts can’t predict yours
After that window, the new-data well runs dry. You’ve mapped your staples and the CGM stops surprising you
The medical critics are right that CGM data is not a substitute for HbA1c in non-diabetics
Beyond the learning window, the CGM is useful for two things: behavioral accountability (the Hawthorne effect) and early warning on metabolic shifts or drug/supplement side effects
Month one: your personal nutrition map
The first month is where the value lives. The Stanford “glucotypes” study put CGMs on 57 mostly healthy people and found 80% spiked to prediabetic or diabetic glucose levels after eating cornflakes with milk (PLOS Biology, 2018; observational, n=57). The lead researcher’s takeaway: “There are lots of folks running around with their glucose levels spiking, and they don’t even know it.”
The Weizmann Institute tracked 800 participants wearing CGMs for a week, measuring 46,898 meals, and found 5x variation in glycemic response to identical foods between individuals (Zeevi et al., Cell, 2015; observational cohort, n=800). A 2025 study confirmed it: each person has a carbohydrate “fingerprint,” and rice-spikers are more likely to be Asian, which, given my own CGM history, was not exactly a surprise (Wu et al., Nature Medicine, 2025; crossover, n=55).
That variance is the whole reason population nutrition charts fail you. A “low-GI” food is an average across hundreds of people. You might respond very differently to the same food compared to your friend.
So what do you do? Here’s how to spend four weeks with the device.
Week 1: log meals and watch the spikes. What you eat, when you eat it, what happens to your glucose. The spikes you see in your usual pattern are your baseline.
Weeks 2-4: experiment. Some worth testing:
Eating vegetables and protein first, vs starting with rice or roti
Building out the plate (more fiber, vegetables, healthy fats, protein), vs starchy carbs alone
Different starch sources (rice, roti, oats, potato) to see which one spikes you most
A 15-20 min walk after a meal, vs sitting on the couch
10 squats every hour during a long sitting day, vs sitting straight through
If you are tracking your sleep, see how a good night’s sleep impacts the next day
A teaspoon of psyllium husk (Isabgol) 30 minutes before the meal
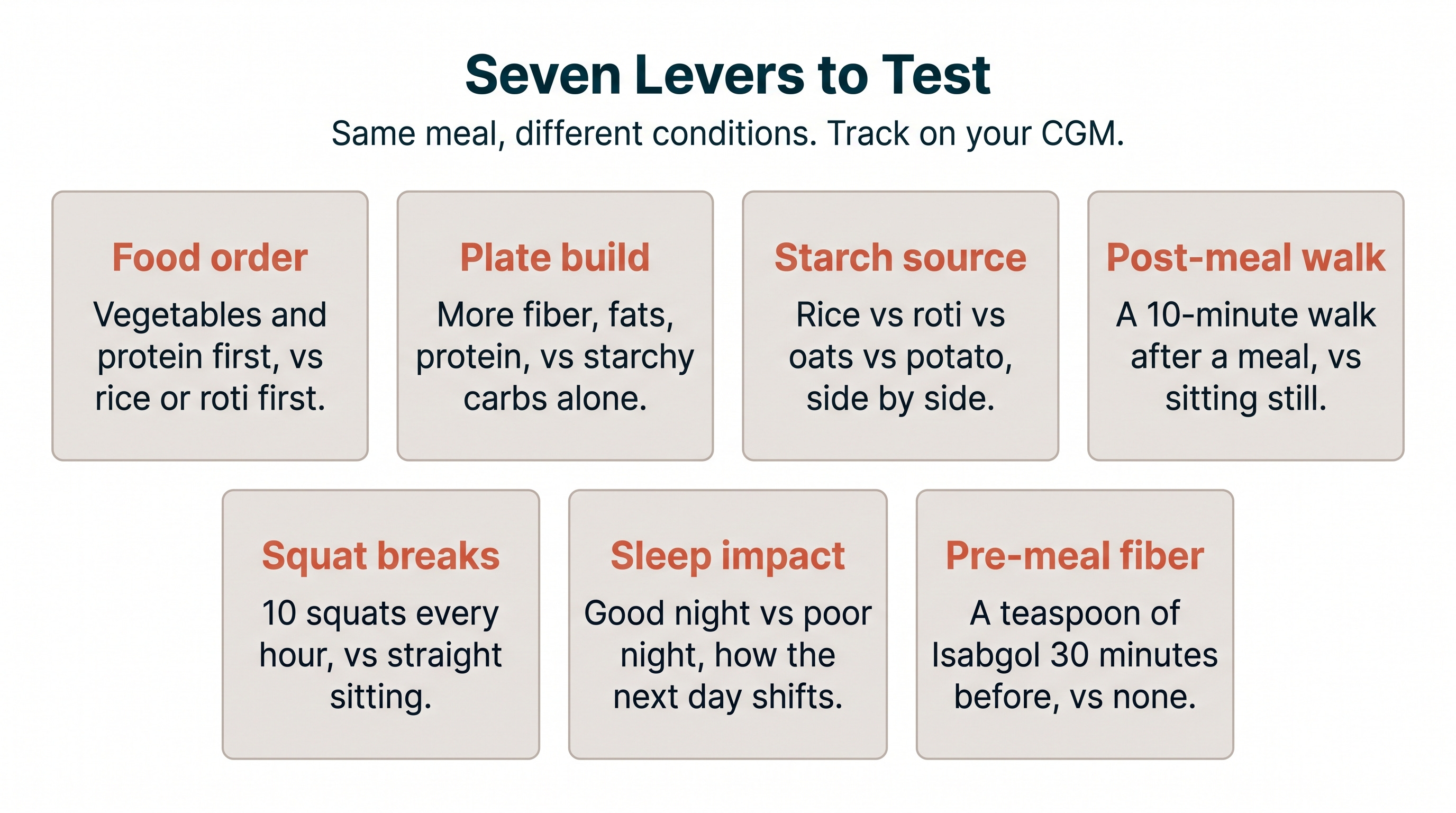
You’ll see which foods consistently spike you, which conditions blunt the spike or cause it to come down quickly, and which interventions actually moved the needle. That’s your personal guide.
After month one: the diagnostic limits
The educational value has a natural end. Once you’ve cycled through your regular foods, the spikes stop being news. You learn how you respond to dal-chawal, your usual breakfast, your post-workout snack. After that, the CGM is showing you variations on patterns you already know.
This is also where the medical critics are right. A 2025 Mass General Brigham study of 972 adults found that CGM metrics correlated well with HbA1c in people with type 2 diabetes, weakly in prediabetes, and showed essentially no correlation in people with normal blood sugar (Diabetes Technology and Therapeutics, 2025; observational). University of Bath researchers found CGMs overestimated “time above range” by nearly 400% compared to gold-standard finger-prick tests in healthy adults, and misclassified low-GI fruits as medium or high-GI (American Journal of Clinical Nutrition, Feb 2025). The lead author explained the gap simply: CGMs measure glucose in the interstitial fluid around your cells, not in your blood, which introduces lag and inaccuracy at the edges.
The critics are evaluating the CGM as a diagnostic tool. As a diagnostic tool for healthy adults, it doesn’t really work, and the error rate is part of why. CGMs are accurate enough for someone whose glucose swings from 80 to 250, because the device’s error band is small relative to the signal. In a healthy adult whose glucose lives between 80 and 140, that same error band is large enough to make a normal post-meal reading look like a spike, or vice versa. The 400% overestimate is what happens when you push an interstitial-fluid sensor into a range it wasn’t optimized for. For most people, the natural endpoint is somewhere around four to six weeks. They’ve learned what they came to learn, and the device has nothing new to add.
Keep it on for accountability
For some people, including me, there’s a second reason to keep wearing it. It’s the Hawthorne effect: when people know they’re being observed, their behavior shifts toward what they think they should be doing. The data doesn’t have to be new for the device to keep working on you.
When my CGM is on, I eat fewer carbs at night, I snack less, I make better choices because I know the data is there, recording everything. When I take it off, I drift. I’ve tested this multiple times over five years. The pattern is consistent. I hate seeing big spikes on the graph, which makes me eat differently.
The same dynamic shows up in daily weighing. A study of 9,768 smart scale users found that only daily weighing was associated with weight loss across all BMI groups (JMIR, 2021; observational cohort, n=9,768). When participants stopped weighing for 30 or more days, they gained an average of 0.85 kg. The mechanism is identical: awareness triggers self-evaluation, which triggers corrective action.
If that kind of accountability is helpful for you, the CGM can be a very useful tool for blood sugar control. If it isn’t, or if it nudges you toward food anxiety instead of better choices, it’s the wrong tool.
Keep it on for early warning
There’s a third reason some people keep wearing one. When I started rosuvastatin (Crestor), I noticed within two weeks that my glucose spikes were getting larger and taking longer to come back down. Statins are known to increase insulin resistance by approximately 24%, with the pancreas trying to compensate until the system tips toward type 2 diabetes (ATVB, 2021). But HbA1c takes two to three months to reflect those changes. My CGM showed the shift in 14 days. I caught a real drug side effect months before my next blood draw would have flagged it.
Separately, I was waking up at 5am every morning for weeks without understanding why. When I looked at my overnight glucose traces, the pattern was obvious. My glucose was dipping in the early morning hours, triggering a cortisol and adrenaline response that pulled me awake (peak window for nocturnal hypoglycemia is between 04:00 and 07:30). I started having a piece of fruit with cottage cheese about an hour before bed, and the early wake-ups stopped within days.
Neither of those would have shown up on a standard lab panel. Postprandial glucose abnormalities can appear years before fasting glucose and HbA1c start to drift, and CGM is the practical way to see them (Journal of Multidisciplinary Healthcare, 2024; review). For South Asians, who develop metabolic dysfunction at lower thresholds, catching these shifts early may matter even more. A 2025 study found CGM metrics could differentiate prediabetes from normoglycemia in Asian individuals even when fasting glucose appeared normal (Chandran et al., Journal of Diabetes Science and Technology, 2025; observational).
Myth: “If you don’t have diabetes, a CGM is a waste of money”
The Myth: CGMs are medical devices for managing diabetes. If your blood sugar is normal, wearing one is expensive wellness theater, paying $100 a month to watch numbers that don’t mean anything clinically.
The Evidence: The belief persists because CGMs were marketed as optimization tools by wellness companies, and endocrinologists rightly pushed back on that framing. The critics are right about the diagnostic claim. But they’re evaluating only one of the device’s possible uses. The first four to six weeks of CGM data are genuinely educational for most people, regardless of diabetes status, because individual glycemic variability is large enough that you cannot predict your response to a food from population averages. After the learning window, the CGM becomes optional. For some people, behavioral accountability (the same psychology that makes daily weigh-ins work for weight loss) makes the cost worth it. For others, early detection of drug side effects or metabolic shifts justifies keeping it on. Most people probably should wear one for a month, learn what they came to learn, and take it off.
The Verdict: The first four weeks are worth it for almost anyone. After that, only if the accountability or early warning value is something you specifically need.
The CGM is a small example of a bigger pattern. Personal data lets you stop arguing with averages. Once you know how your body responds, you stop needing somebody else’s chart. The first month of wearing one is the lesson. What you do after is yours to decide.
How to Try One
You don’t need a prescription anymore. Dexcom Stelo (~$99/month for two 15-day sensors) and Abbott Lingo (~$49 for two weeks, $89 for four) are both OTC and ship directly from the company. Pick one, wear it for a month, run your food experiments. If you’re already on medications that affect glucose (statins, steroids, beta-blockers) or you have a family history of diabetes, loop your doctor in so the data lives in your file. Otherwise, the barrier to entry is lower than it’s ever been. OTC CGMs are slightly less accurate than prescription versions, but unless you have a metabolic diagnosis or risk flag, most doctors won’t prescribe one and insurance won’t cover it. For a one-month learning experiment, OTC is the path.
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.