
Do Natural Alternatives to Statins Work?
The different options, the data behind them, and what really makes a difference.

A naturopathic doctor recommended red yeast rice to me a few years ago. “Natural cholesterol lowering,” they said. “Better than a statin.” I took it for a while. Then my liver enzymes climbed, I stopped, and they came down. That was the first clue. Looking back, I was lucky it stopped at liver enzymes.
The second came when I looked up what was actually in the bottle. The active ingredient in red yeast rice is monacolin K. Monacolin K is chemically identical to lovastatin, a prescription statin. The “natural alternative” IS the drug, sold without the dosing consistency, purity testing, or regulatory oversight that the prescription version requires. When researchers tested twelve red yeast rice products, they found citrinin, a toxic mycotoxin linked to kidney damage, in four of them (Gordon et al., Archives of Internal Medicine, 2010; laboratory analysis).
That sent me down a rabbit hole on every supplement marketed as a statin replacement, and I applied the same question from Part 1: has this been proven to prevent heart attacks, or does it just move a number on a lab report? For almost all of them, the answer is “the second.” For one, the answer is different. Let me show you both.
The Bottom Line
No “natural statin alternative” has a single large RCT showing it prevents heart attacks or strokes
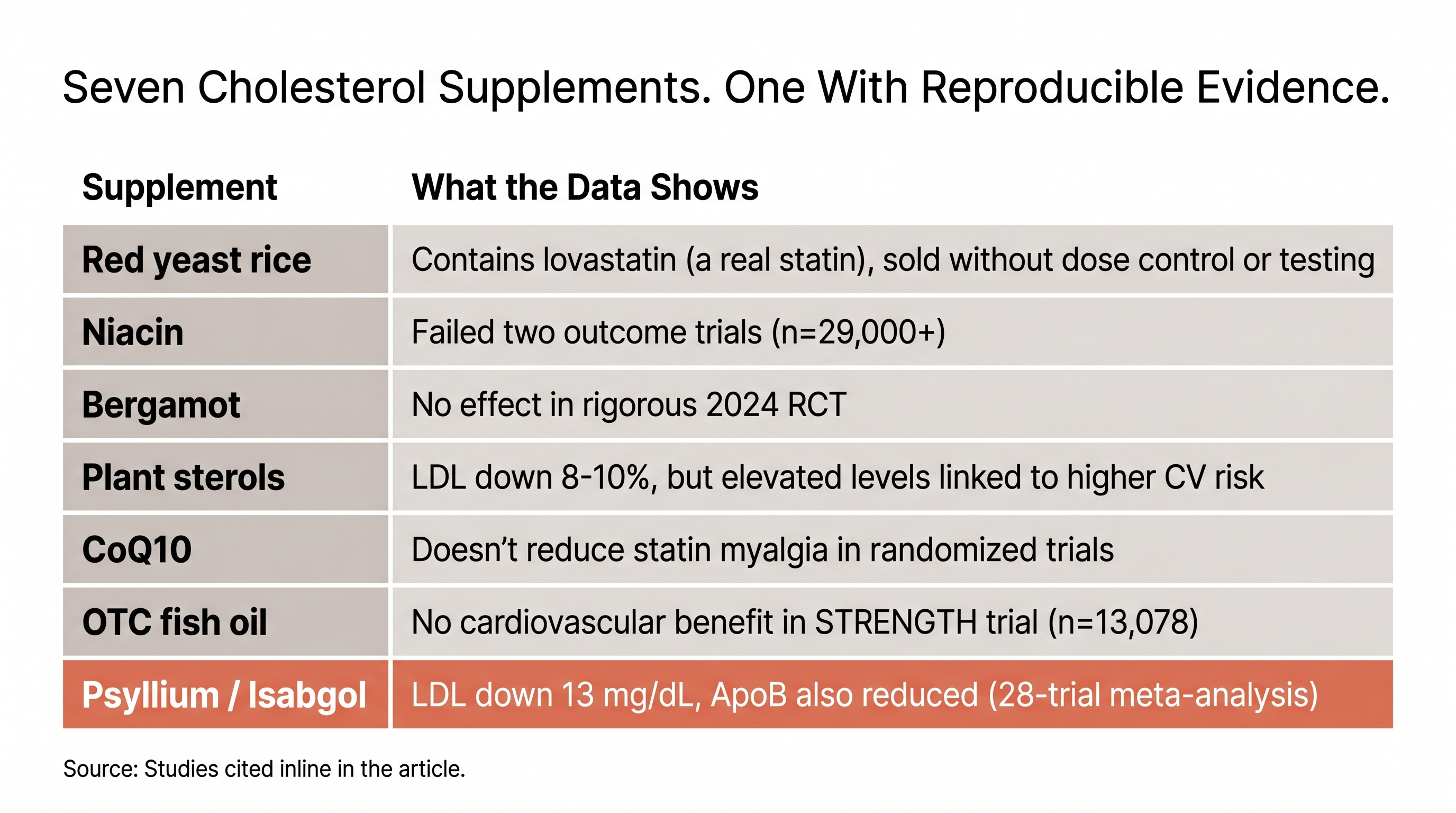
Red yeast rice IS lovastatin (a prescription statin) in unregulated form, with toxic contamination in 4 of 12 products tested
Niacin was tested in 25,673 patients and caused more harm than benefit. Two large trials ended the enthusiasm.
The FDA identified 776 supplements containing unapproved pharmaceutical ingredients from 2007-2016
Psyllium is the one exception: real LDL and ApoB data, boring mechanism, part of my regimen. Covered in a dedicated section below.
If your red yeast rice “works,” you’re taking an unregulated statin
The paradox sharpens when you follow it to its conclusion: if your RYR product has enough monacolin K to lower your LDL, you’re taking a statin with no quality control over dose, purity, or contamination. If it doesn’t contain enough, it’s doing nothing.
The chemical identity isn’t a coincidence. The first statin was discovered in 1973, when a Japanese biochemist named Akira Endo isolated it from a Penicillium mold growing on rice at a Kyoto grain shop. Red yeast rice is rice fermented on a different fungus that makes monacolin K, a molecule structurally identical to lovastatin. Both came from fungi making compounds that block the same enzyme. What separates them is regulation: dose, purity, and outcome data.
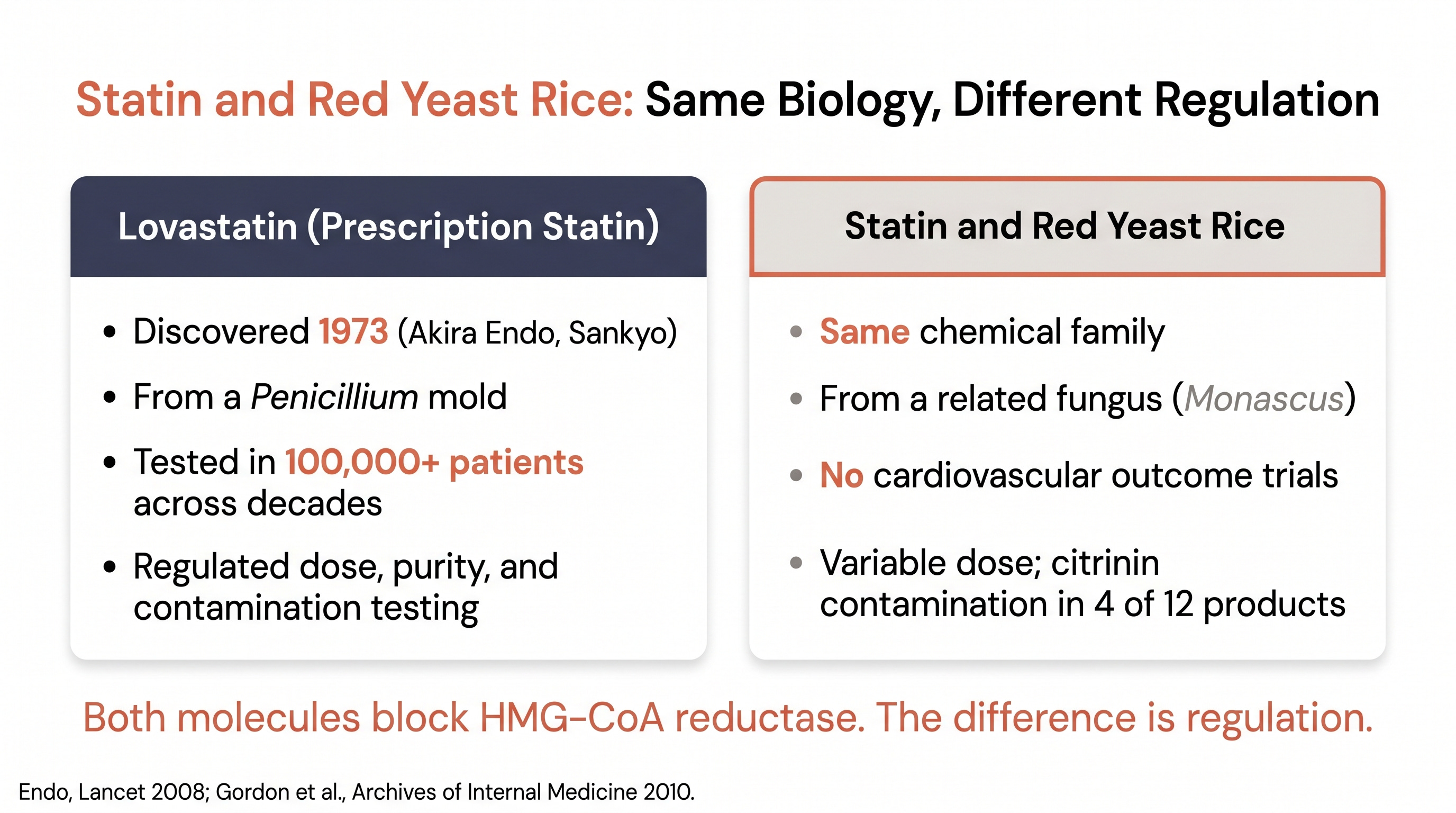
The FDA recognized this two decades ago, ruling Cholestin (a popular RYR supplement) an unapproved drug in 1998 and warning consumers about unauthorized lovastatin in RYR products in 2007. The monacolin K content varies wildly across brands, which means your dose changes every time you open a new bottle. That citrinin contamination in 4 of 12 products isn’t a theoretical concern either. Citrinin is a mycotoxin linked to kidney damage.
The clinical evidence behind RYR is thin. The studies are small, short, and none have measured cardiovascular outcomes like heart attacks or strokes. Compare that to the statin outcome data from Part 1: over 100,000 patients across decades of randomized trials.
Here’s the practical absurdity: generic lovastatin costs $4-10/month with a prescription. It comes with regulated dosing, known purity, and decades of safety monitoring. The RYR supplement that contains the same molecule often costs more, with none of those guarantees.
Niacin had its chance. Two large trials ended it.
Niacin is the cautionary tale for this entire conversation. For years it was a mainstream cholesterol therapy, prescribed to raise HDL. Unlike most supplements on this list, it got tested in large, rigorous trials, and failed both.
AIM-HIGH (NEJM, 2011; RCT, n=3,414) tested extended-release niacin added to statin therapy. No reduction in cardiovascular events. The trial was stopped early for futility. HPS2-THRIVE (NEJM, 2014; n=25,673) was even more definitive: niacin plus laropiprant added to statin therapy showed no cardiovascular benefit and caused more side effects, including infections, bleeding, and new-onset diabetes.
Two trials, nearly 30,000 combined patients. Niacin improves the HDL number on your lab report. It does not prevent heart attacks.
Four more supplements, zero cardiovascular outcome data
Bergamot doesn’t work in rigorous trials. The 2024 placebo-controlled RCT (MDPI Foods, 2024; n=110) found no improvement on LDL or oxidative stress markers, despite earlier excitement from small Italian studies. No cardiovascular outcome data exists.
Plant sterols are the strangest case. They produce a real 8-10% LDL reduction, but Mendelian randomization studies have linked elevated circulating plant sterols with cardiovascular risk (Nutrients, 2023). Lowering LDL through this mechanism may not deliver the benefit the LDL drop implies, and no outcomes trial has tested whether it does.
CoQ10 is the most common “take this with your statin” recommendation, and the evidence doesn’t support it. The premise is logical (statins block CoQ10, so supplementing should reduce muscle pain), but meta-analyses of randomized trials show it doesn’t help (JAHA, 2018; n=1,776). The deeper finding from one NIH-funded trial: only 36% of patients with self-reported statin myalgia developed symptoms during blinded testing. The other 64% were reacting to the idea of the drug.
Over-the-counter fish oil isn’t the same as Vascepa. The STRENGTH trial (JAMA, 2020; RCT, n=13,078) of EPA+DHA combo found no cardiovascular benefit. Vascepa is a prescription purified EPA with outcome data from REDUCE-IT, but it’s a regulated drug, not a supplement.
Psyllium is the exception
Before closing the door on supplements entirely, one deserves a section of its own. Psyllium husk, what most South Asian households know as Isabgol, is the one supplement in this category with real LDL and ApoB data.
A meta-analysis of 28 trials found that 10.2g daily reduced LDL by an average of 13 mg/dL and also reduced ApoB (Jovanovski et al., American Journal of Clinical Nutrition, 2018; n=1,924). The mechanism is physical: psyllium forms a viscous gel in your gut that binds bile acids. Your liver, now short on bile acids, pulls cholesterol out of circulation to make more. The result is a reliable LDL drop that compounds when paired with other lipid-lowering therapy.
This is category-different from the supplement graveyard. It’s fiber: cheap, boring, and effective. It’s been part of my own regimen for over a year. Practical basics: 10g daily, mixed in a full glass of water, before meals. For the full protocol, brand selection, and the synergy with Zetia, see my deeper write-up on psyllium.
776 supplements, and nobody had to prove they worked first
The Dietary Supplement Health and Education Act of 1994 makes all of this possible. Under DSHEA, supplements don’t have to prove they’re effective or safe before being sold. The FDA can only act after harm has already been demonstrated.
The consequences are measurable. The FDA identified 776 supplements containing unapproved pharmaceutical ingredients between 2007 and 2016 (JAMA Network Open, 2018; regulatory analysis). Roughly 20% of those contained multiple unapproved drugs. A separate analysis across 13 countries found 14.8% of non-hormonal supplements contained undeclared anabolic steroids. Independent testing by ConsumerLab has found roughly one in three multivitamins fail quality standards.
I wouldn’t run a business without audited financial data. At some point I started asking myself whether I was applying the same standard to my cardiovascular health.
“The ‘natural is safer’ belief is one of the most stubborn things I hear in clinic, especially from South Asian patients whose families have been reaching for ayurvedic or herbal options for generations. The intention is good. The evidence is not. When a product moves LDL but has no outcome data, we are betting on a lab number instead of a life. Psyllium is the one adjunct I recommend broadly. Everything else in this category needs outcome trials before I would put it on a patient’s chart.”
- Dr. Karan Bhalla
What absence of evidence actually means
To be fair, absence of evidence is not evidence of absence. Large cardiovascular outcome trials cost hundreds of millions of dollars, and without patent protection, no supplement manufacturer has the incentive to run one. That’s a real limitation of the system, not a mark against any individual product.
But the limitation doesn’t change the evidence standard. If you’re choosing between a treatment proven to prevent heart attacks in tens of thousands of patients and one that hasn’t been tested at that level, the gap is real regardless of why it exists.
Myth: “Natural supplements are safer than prescription drugs”
The Myth: Natural alternatives to statins are safer because they come from nature, have fewer side effects, and aren’t made by pharmaceutical companies.
The Evidence: Red yeast rice IS a pharmaceutical (lovastatin) sold without pharmaceutical quality control, with toxic citrinin contamination in 4 of 12 products tested (Archives of Internal Medicine, 2010). Niacin, when tested in a large trial (HPS2-THRIVE, n=25,673), caused more infections, bleeding, and new-onset diabetes than placebo. The FDA found 776 supplements with undisclosed pharmaceutical ingredients (JAMA Network Open, 2018). Meanwhile, generic statins ($4-10/month) have decades of safety data in over 100,000 patients, known side effect profiles, and regulatory oversight requiring ongoing adverse event reporting.
The Verdict: “Natural” is a marketing category, not a safety category. Unregulated supplements have less safety data, less quality control, and in some cases more dangerous contamination than the prescription drugs they claim to replace.
One Thing I Changed
The RYR experiment ended my curiosity about cholesterol supplements. Psyllium earned its place in my regimen; the rest went back to the shelf. When I read a supplement label now, I read it for what’s missing as much as what’s listed: the outcome data, the dose consistency, the contamination testing. That’s usually where the story is.
Bring the supplement bottle with you
When you see your doctor, bring the actual bottle of any supplement you are taking for cholesterol. Not the name, the bottle. Let them read the label, the dose, and the ingredient list. For red yeast rice specifically, ask whether the monacolin K content is disclosed, and whether the product has been tested for citrinin. For anything else claiming to lower cholesterol, the question is simple: has this been shown to prevent heart attacks, or just to lower a number? Psyllium is the one adjunct I feel comfortable recommending across the board. The rest of this category belongs in a different conversation, one about evidence, not tradition.
- Dr. Karan Bhalla
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.