
Do Statins Cause Diabetes?
A little. And it prevents five times more heart attacks than it causes.


I kept hearing it from family, from South Asian health communities, from Reddit threads that confidently cited “the studies”: statins cause diabetes. I half-believed it, and my Mom said the same about her own diagnosis. When my rosuvastatin started pushing my fasting insulin and A1c in the wrong direction, I thought I had my answer.
Then I looked at the actual data and realized I was asking the wrong question. “Do statins cause diabetes?” sounds like it has a yes or no answer. It doesn’t. The useful questions are different, and they changed how I think about this decision and about health decisions in general.
The Bottom Line
“Do statins cause diabetes?” is the wrong question. Three better ones: what’s the tradeoff, which statin, and what’s the real alternative?
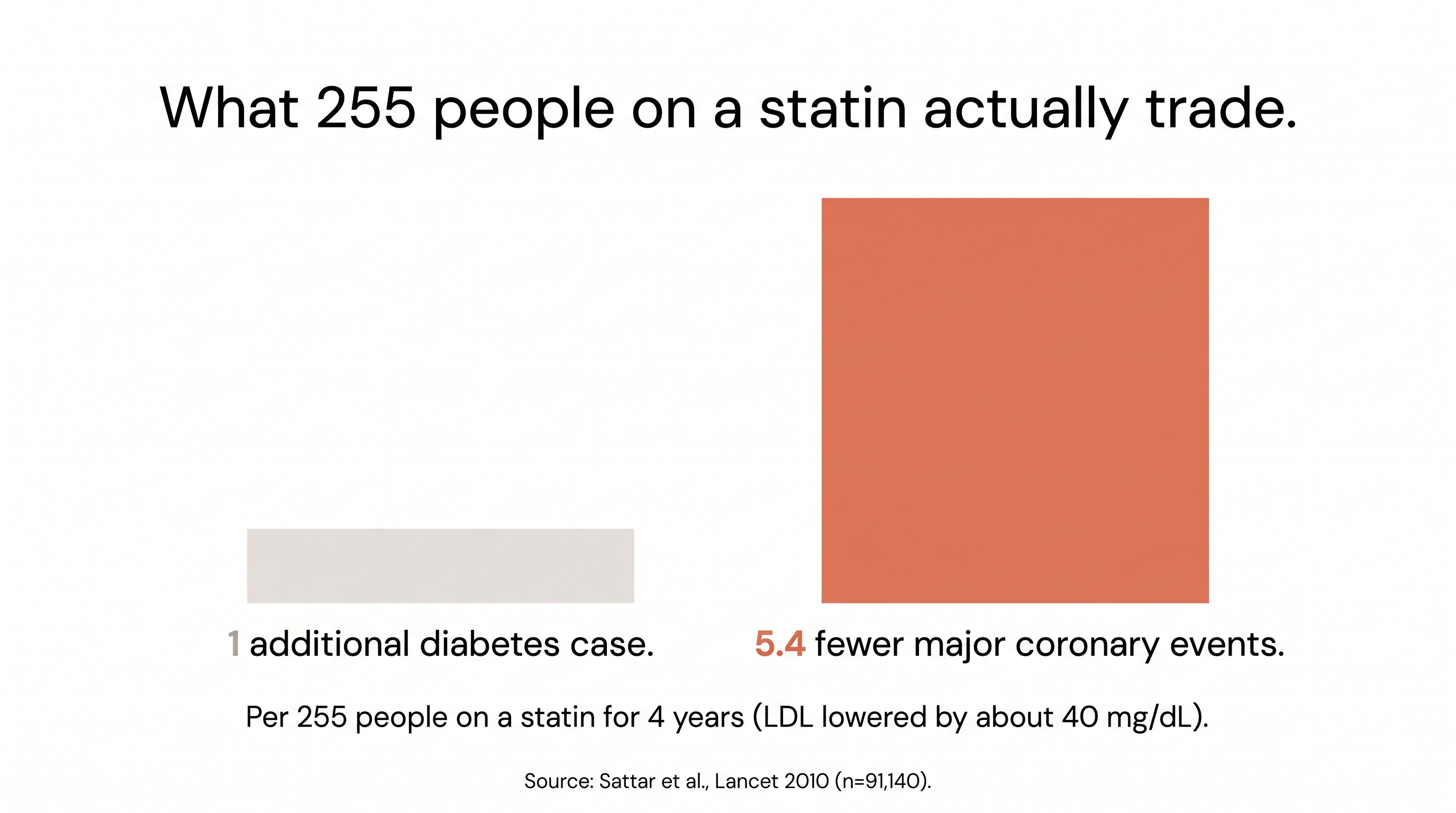
The tradeoff: for every 1 diabetes case, 5.4 cardiovascular events prevented. 62% of new cases occur in people already near the diabetes threshold.
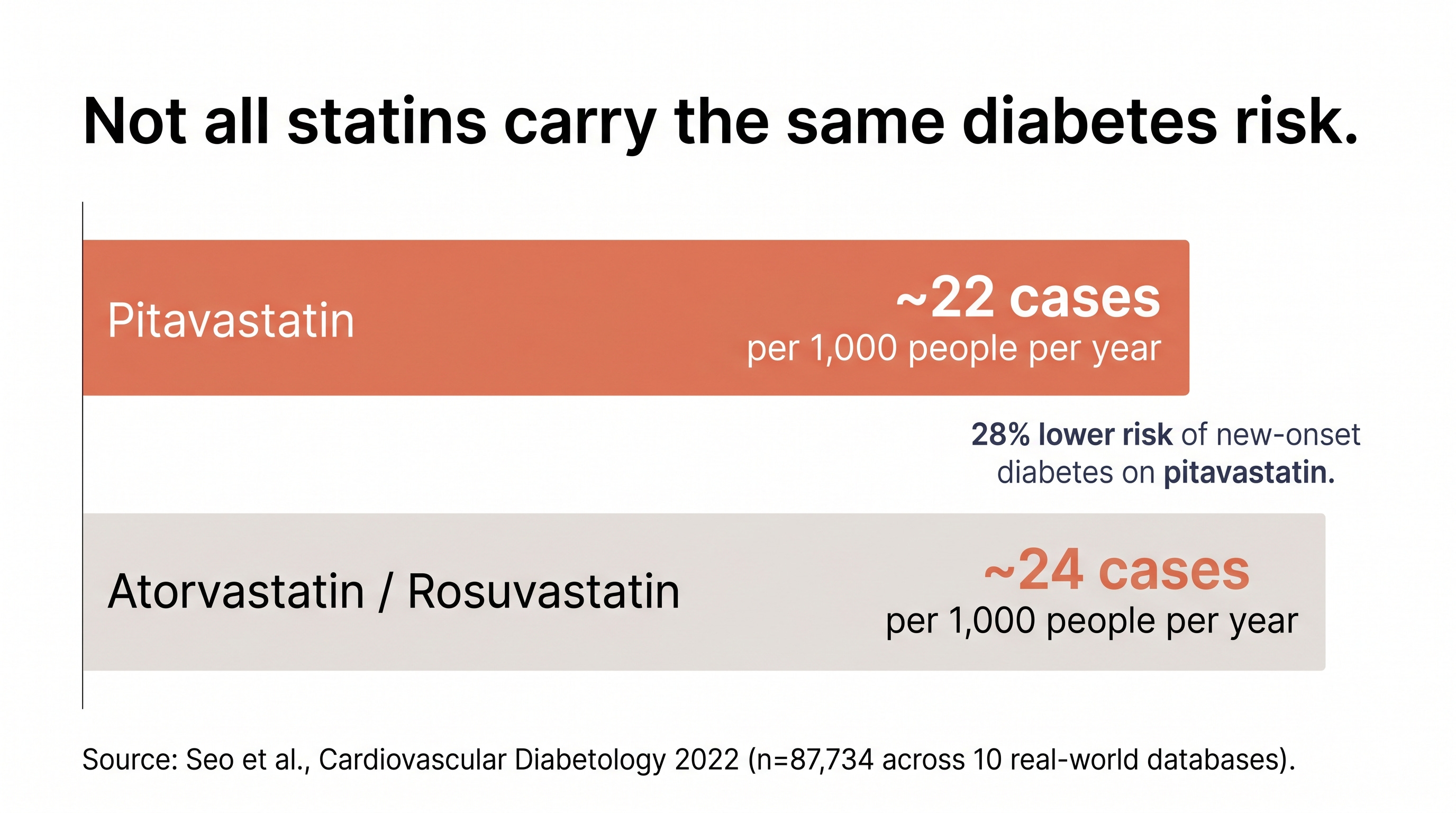
Not all statins are equal: pitavastatin is glucose-neutral, atorvastatin carries the highest risk
No supplement (red yeast rice, berberine, bergamot, niacin) has cardiovascular outcome data
For every diabetes case, five cardiovascular events don’t happen
The fear is real. Statins do increase diabetes risk. The largest meta-analysis on this, covering 13 trials and 91,140 patients, found a 9% relative increase in new-onset diabetes (Sattar et al., Lancet, 2010; meta-analysis, n=91,140). Over 4 years, for every 255 people treated, 1 additional diabetes case. But for every roughly 40 mg/dL drop in LDL, those same 255 people experienced 5.4 fewer major coronary events (heart attacks and coronary deaths). The ratio is 5:1 in favor of treatment, and it gets wider once you add in strokes and revascularizations.
The randomized evidence tells the same story. JUPITER, a trial that prospectively tracked diabetes alongside cardiovascular outcomes, randomized 17,603 people without diabetes to rosuvastatin 20mg or placebo (Ridker et al., Lancet, 2012; RCT, n=17,603). Rosuvastatin produced 270 new diabetes cases vs. 216 on placebo, a 25% relative increase. But the risk concentrated in people with baseline metabolic syndrome, impaired fasting glucose, BMI of 30 or higher, or HbA1c above 6%. In those without any of those risk factors, diabetes incidence was unchanged.
The 2024 CTT update made the picture even clearer. Using individual participant data from large, double-blind RCTs, it found that 62% of new diabetes cases occurred in people already in the top quarter of baseline glucose (CTT Collaboration, Lancet Diabetes & Endocrinology, 2024). The HbA1c increase was 0.06-0.08%, which is clinically trivial. The people developing diabetes on statins were already approaching the threshold, and the statin pushed them over a line they were walking toward. “Statins reveal diabetes” is closer to the truth than “statins cause diabetes.”
Here’s what makes this personal for anyone reading this newsletter: the people most at risk for statin-induced diabetes (those with prediabetes, metabolic syndrome, visceral obesity) are the same people who benefit most from statins, because their baseline cardiovascular risk is highest.
For South Asians specifically, the Pooled Cohort Equation underestimates our risk by more than 2-fold (predicted 4.8% vs. actual 6.8% 10-year ASCVD rate; Patel et al., Circulation, 2021; UK Biobank, n=8,124 South Asian within a cohort of 458,000). We develop coronary artery disease roughly 10 years earlier than white populations (and if you’re South Asian reading this, that math probably applies to your family too). The 5:1 ratio for a general population is probably more favorable for us, though we lack the ethnic-specific trial data to prove it.
Any time someone tells you a medication “causes” something, ask what’s on the other side. The scary number without the benefit number is half a story.
“When a South Asian patient comes in worried about statins and diabetes, I show them the ratio and the baseline-glucose data. The diabetes risk is real, but it is concentrated in people already near the threshold, and the cardiovascular benefit is larger for us than for the average trial population. For patients with prediabetes or metabolic syndrome, I often reach for pitavastatin or a moderate-intensity statin paired with ezetimibe rather than a high-intensity statin alone. Same LDL target, less glucose pressure.”
- Dr. Karan Bhalla
Seven drugs, not one
Most people treat “statin” as a single thing. It’s seven different drugs with seven different metabolic profiles.
The diabetes risk varies meaningfully between them. At one end: pitavastatin, which most people haven’t heard of. A distributed network analysis across 10 real-world databases compared pitavastatin to atorvastatin and rosuvastatin and found pitavastatin had a 28% lower risk of new-onset diabetes (Seo et al., Cardiovascular Diabetology, 2022; n=87,734 across 10 databases). Glucose-neutral in practice, effective LDL lowering, available generically.
At the other end, atorvastatin and rosuvastatin carry the highest diabetes risk among commonly prescribed statins. The same Seo analysis found the incidence rate was consistently higher on both than on pitavastatin across all 10 databases.
Dose matters too. High-intensity statins carry a 36% proportional increase in diabetes risk, while low-to-moderate intensity statins carry only 10% (CTT Collaboration, Lancet Diabetes & Endocrinology, 2024). This is a lever you can pull. A moderate-intensity statin combined with ezetimibe achieves similar LDL targets with 18% less diabetes risk than a high-intensity statin alone (pooled meta-analysis of 4 cohort studies). Same destination, different metabolic cost.
Which one? At what dose? Combined with what? Those are the questions that matter when a statin is on the table.
Your supplement hasn’t been tested against a heart attack
The instinct to try something natural first is understandable. I’ve had that conversation in my own family. But when someone chooses berberine over a statin, or red yeast rice over rosuvastatin, they’re making an evidence decision whether they know it or not. The question is: what standard of proof am I requiring before I bet my cardiovascular health on it?
Statins have cardiovascular outcome data in over 100,000 patients across decades of randomized trials. No supplement, not red yeast rice, not berberine, not bergamot, not niacin, has a single large RCT showing it prevents heart attacks or strokes. Some move a number on a lab report. None have been proven to prevent the event that number is supposed to predict.
What the statin-type ranking can’t tell us yet
The head-to-head diabetes risk comparison across statins comes primarily from observational data and network analyses, not from randomized trials designed to compare one statin against another on metabolic outcomes. The pitavastatin data is encouraging but based on smaller populations than the atorvastatin and rosuvastatin evidence. And South Asians are underrepresented in nearly all major statin trials, which means the ethnic-specific tradeoff ratio (likely more favorable than 5:1) is estimated, not proven. The direction of the evidence is clear. The precision will sharpen as more data comes in.
Myth: “Statins cause diabetes, so you’re trading one disease for another”
The Myth: Taking a statin means trading heart protection for a new metabolic problem. The diabetes risk cancels out the cardiovascular benefit.
The Evidence: The “trade” framing assumes the two risks are equivalent. They aren’t. The cardiovascular events statins prevent (heart attacks, strokes, cardiovascular death) are acute and often irreversible. The diabetes cases statins contribute to are concentrated in people who were already metabolically close to the threshold, with HbA1c increases of 0.06-0.08%, manageable with monitoring and lifestyle. One side of the trade is catastrophic. The other is a lab value that crossed a line it was approaching anyway. The 5:1 ratio covered earlier quantifies this: the benefit outweighs the risk by a wide margin, and the risk itself is not the diabetes most people picture when they hear the word.
The Verdict: The risk is real, but calling it a “trade” overstates the diabetes side and understates the cardiovascular side. The better question: which statin, at what dose.
One Thing I Changed
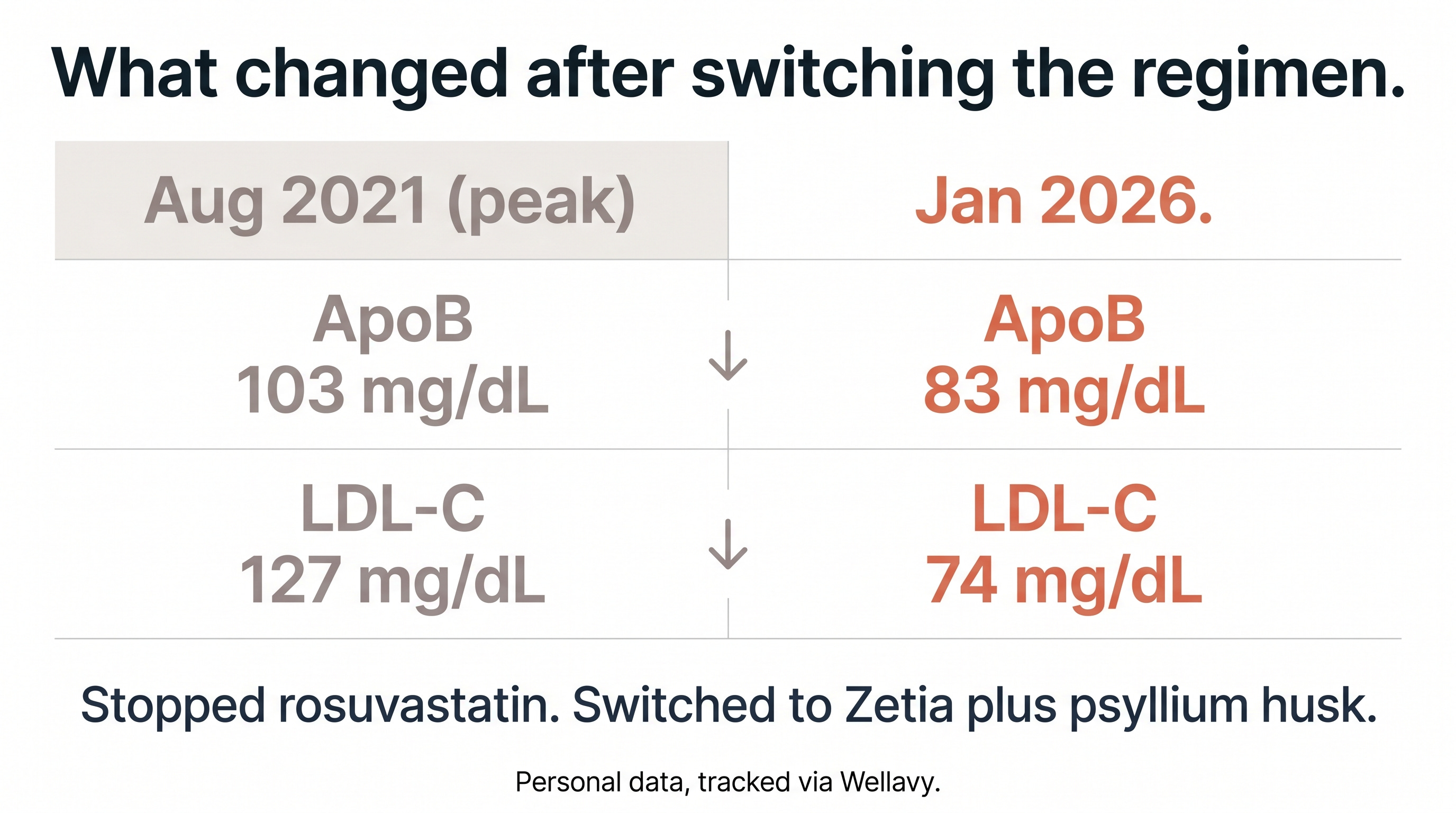
I stopped my rosuvastatin after it raised my fasting insulin and A1c. I did not stop lowering LDL. Zetia plus psyllium husk carried the work for over a year, dropping my ApoB from a peak of 103 to 83 and LDL from 127 to 74. I just switched to Repatha, a PCSK9 inhibitor. Early days. I’m waiting for the numbers to settle before deciding what the long-term regimen looks like.
The framing shift is what stuck with me. Yes-or-no rarely fits a health decision. The questions that do, and that I now bring to every one: what’s the tradeoff, which intervention, and what’s the real alternative.
Choose the statin, not just whether to take one
Before you start or stop a statin, ask which one and at what dose. Not all statins are the same. For my South Asian patients with prediabetes or metabolic syndrome, I often recommend pitavastatin or a moderate-intensity statin combined with ezetimibe rather than a high-intensity statin alone. Same LDL target, less glucose pressure. If the diabetes signal worries you, the path forward is granular: pick the right agent, the right dose, and the right combination.
- Dr. Karan Bhalla
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.