
Is Ghee Good or Bad?
There's no one right answer on ghee. Here's how to find yours.


This week’s issue features a guest perspective from Dr. Neil Parikh, CEO of DOC, former CMO of Thirty Madison.
Every South Asian family has some version of this argument. The aunties swear by ghee (loudly). The cardiologists say cut it. The internet is split between “ancestral superfood” and “arterial poison.”
I am a Punjabi and grew up in Delhi, with ghee in our kitchen. In the parathas, on the dal, stirred into the rice. It was love on the plate. So when I started looking at the evidence, I wanted a real answer.
“My grandmother loved cooking with ghee and always has. Every time we would visit, she would feed us home-cooked food with lots of ghee in it. My mom, on the other hand, took a different approach and believed that ghee was the root of the cholesterol evil, and our food at home was not cooked in ghee. I still remember the disappointment my grandmother expressed in my mom’s cooking.”
- Dr. Neil Parikh, CEO of DOC, former CMO of Thirty Madison
The largest meta-analysis ever done on ghee and heart disease screened 919 articles and pulled 18 studies covering nearly 20,000 people, roughly 4,500 of them from the Indian subcontinent (Progress in Nutrition, 2025; systematic review and meta-analysis, n=19,948). The result was wide enough to mean “slightly protective” or “slightly harmful” or anything in between.
After all that data, the most honest thing science can say is: it depends. And that “it depends” pointed me somewhere useful.
TL;DR
Whether ghee raises your numbers depends on your phenotype, your plate, and your labs, not on population averages.
The 2025 meta-analysis (n=19,948) found no significant heart disease risk from ghee on average. Averages mask wide individual variance.
A 2022 crossover RCT (n=30) showed ghee raised ApoB by +9 mg/dL vs olive oil on average. Your response could be very different.
Hyperproducers vs hyperabsorbers explains the variance. A sterol panel tells you which you are.
919 articles later, science shrugged
That wide range is a shrug. The cleanest direct comparison sharpens the picture a little. A crossover RCT compared ghee against olive oil for four weeks each and found ghee raised ApoB by +9 mg/dL and non-HDL cholesterol by +20.5 mg/dL, both statistically significant (British Journal of Nutrition, 2022; crossover RCT, n=30).
ApoB is the atherogenic particle count, the metric that predicts cardiovascular events better than LDL alone. The signal is real, but n=30 over four weeks is an average across a tiny group, not a prescription for any one person.
One reason the population data is so messy: decades of Indian epidemiological research is confounded by vanaspati. Starting in the 1960s, hydrogenated vegetable oil containing up to 40% trans fats was marketed across India as “vegetable ghee.” Many studies on “ghee consumption” never distinguished desi ghee from vanaspati. The most atherogenic dietary fat in history was literally sold under the same name, and in many Indian households, nobody knew the difference. When someone cites Indian studies on ghee, the first question should be: which ghee?
Three levers, all individualized
Three things decide whether ghee is a problem for you: the plate, your biology, and your numbers.
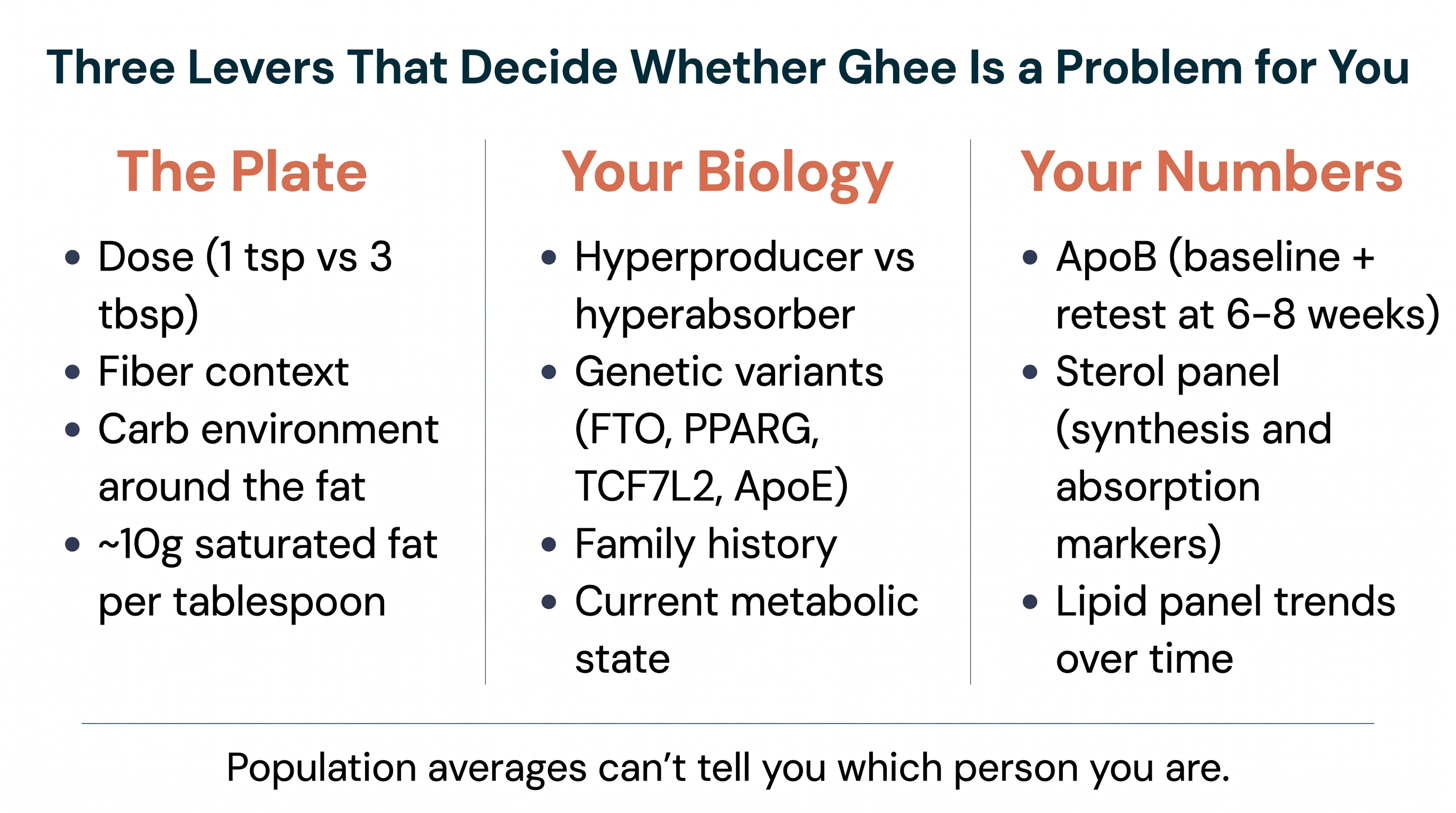
The plate. One teaspoon of ghee finishing a lentil dal is a completely different metabolic event than three tablespoons soaking a paratha with sweet chai. Same fat, different context. The fiber, the dose, the carbohydrate environment around the fat, that’s where the metabolic impact lives.
The numbers add up fast: one tablespoon of ghee delivers roughly 10 grams of saturated fat, half to three-quarters of most recommended daily limits. Traditional Indian cooking often uses two to four tablespoons per dish, and most people aren’t measuring. And many South Asians who “cut ghee” replace it with more roti and more rice, swapping saturated fat for refined carbohydrate, which doesn’t help and often hurts. The plate around the fat matters as much as the fat itself.
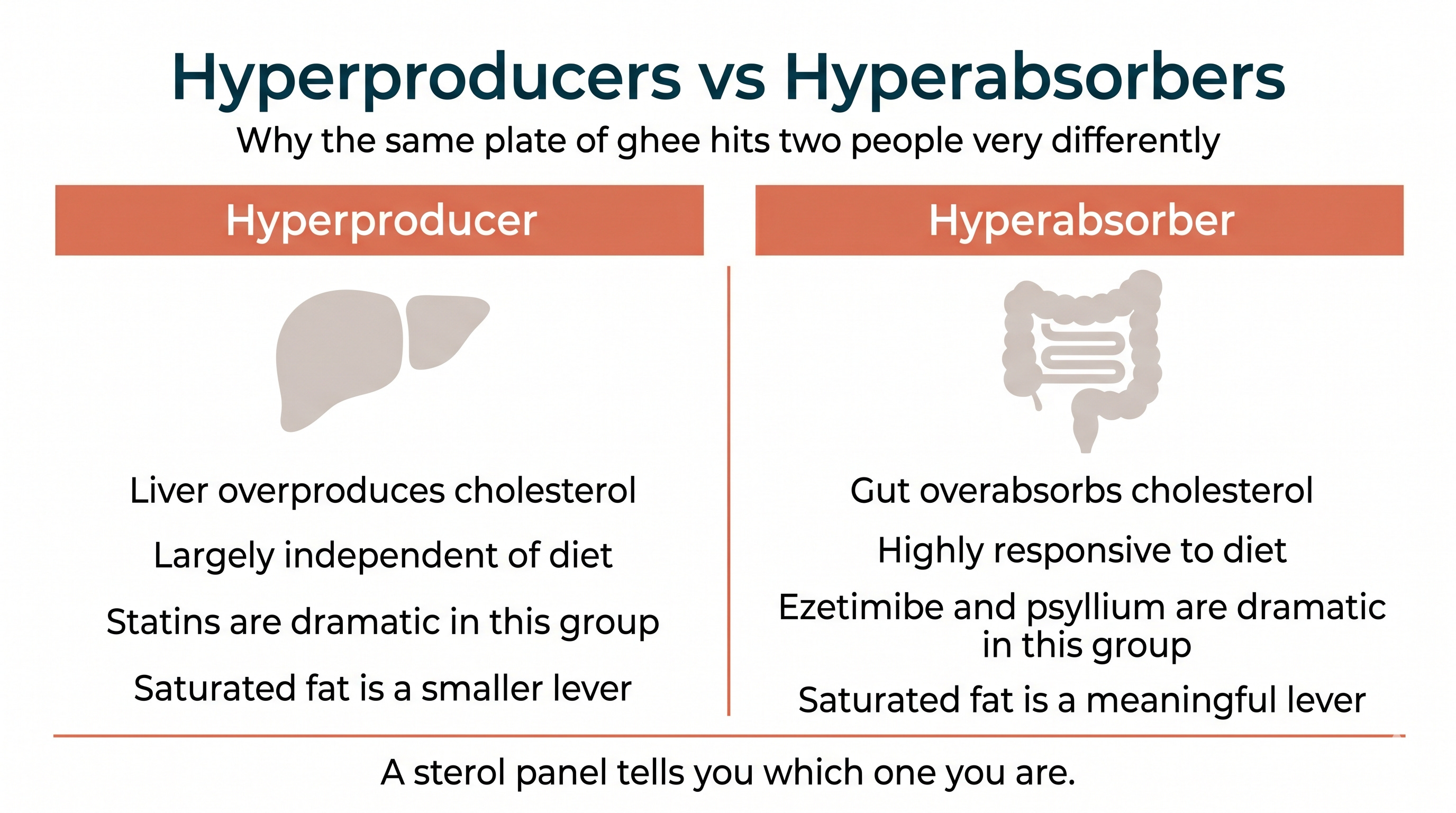
Your biology. The biggest split inside individual biology is hyperproducers vs hyperabsorbers. Hyperproducers make most of their cholesterol in the liver, largely independent of what they eat. Hyperabsorbers pull most of theirs from food and bile through the gut. The same plate of ghee hits these two phenotypes very differently.
It’s the same reason statins (which block production) are transformative for some patients and underwhelming for others, while ezetimibe and psyllium (which block absorption) are dramatic for one group and barely move the needle for another. Psyllium is what most South Asian households know as Isabgol. Dietary saturated fat is on the same axis. Whether ghee raises your ApoB depends on which side of this split you’re on.
Genetic variants (FTO, PPARG, TCF7L2, ApoE), family history, and current metabolic state layer on top of the phenotype. None of them are fully captured by population averages.
“In my clinical practice, saturated fat is one lever among several, and it’s rarely the dominant one. I have hundreds of patients over 300 pounds with near-perfect lipids and no coronary disease. I have lean patients with sky-high ApoB. The variance is wider than population averages suggest. The same way ezetimibe and psyllium dramatically lower cholesterol in some patients and barely move it in others, dietary fat affects different people differently. Your genetics, your family history, and your labs tell you which person you are. At home, we cook with ghee, and use olive oil for dishes that don’t need heat. I do that because I know my numbers. My patients whose labs say otherwise get a different recommendation.”
- Dr. Karan Bhalla
Your numbers. Genetics points the direction, family history sets the risk context, and the labs give the specifics. If you want to go deeper than ApoB, a sterol panel measures synthesis markers (lathosterol, desmosterol) and absorption markers (campesterol, sitosterol), and tells you which side of the hyperproducer / hyperabsorber line you’re on.
My genetic testing flagged a saturated fat intolerance cluster across four gene variants (FTO, PPARG, TCF7L2, PER2), and my father had a heart attack at 69. We swapped ghee for olive oil as our everyday cooking fat. Ghee still shows up for flavor when it matters, but the daily default changed. The swap is a part of a broader lipid management program.
The trial data won’t resolve this for you
The ghee vs olive oil RCT is small (n=30) and short (4 weeks). The meta-analysis is large but inconclusive. Better trials would help, but even a perfect population trial wouldn’t tell you what to do, because population averages hide the responder / non-responder split that’s the whole story.
Your own data already can. Get a baseline lipid panel with ApoB, change one variable, retest in 6-8 weeks. If you want to know the underlying mechanism, get a sterol panel and see which side of the hyperproducer / hyperabsorber line you’re on.
Myth: “Our grandparents ate ghee every day and lived to 90”
The Myth: Ghee has been a staple of Indian cooking for thousands of years. Our grandparents ate it daily and didn’t get heart disease. Modern dietary advice is Western nutrition science ignoring ancestral wisdom.
The Evidence: The ancestral argument cherry-picks one ingredient from a lifestyle package you no longer live. Your grandmother also walked miles a day, ate fewer total calories, consumed far less refined carbohydrate, and had no vanaspati in her kitchen. Ghee existed inside a completely different plate and a completely different life. You can’t isolate one variable and credit it with the outcome.
There’s also survivorship bias at work. You’re remembering the grandparents who lived to 90. Take Neil’s family: all four of his grandparents had heart attacks. India has one of the highest age-standardized CVD mortality rates in the world.
And the study this argument usually rests on (Malhotra’s 1967 observation of 1.15 million Indian railway workers, British Heart Journal, 1967; ecological study) has no individual-level data. Northern India ate more ghee and had less heart disease, but physical activity, urbanization, diet composition, and vanaspati exposure all differed between regions. It cannot establish that ghee prevented anything.
“It’s funny how things come full circle. One day I came home to see my wife, who is American with Irish heritage, cooking with ghee from Whole Foods. I asked her why she was using ghee, and she said, ‘Why not? It’s a superfood.’ It just goes to show how the same food can be considered a superfood in one context and completely evil in another, and how little scientific clarity there is in the broader community.”
- Dr. Neil Parikh
The cultural verdict on ghee depends entirely on where you’re standing. The grandmother who fed it to you, the mom who cut it out, the wife who calls it a superfood. Same ingredient, three opposite stories, all with conviction and none with your data.
The Verdict: It’s Complicated. Both “ghee is poison” and “ghee is fine” are blanket statements that ignore the variance the science actually shows. Your grandparents’ ghee existed inside a lifestyle you don’t live anymore, and “grandma ate it” tells you nothing about your biology. The honest answer for you lives in your labs, not in the culture war.
ApoB before and after, and a sterol panel if you want to go deeper
If you eat ghee regularly and want to know whether it’s a problem for your biology specifically, here’s what I recommend.
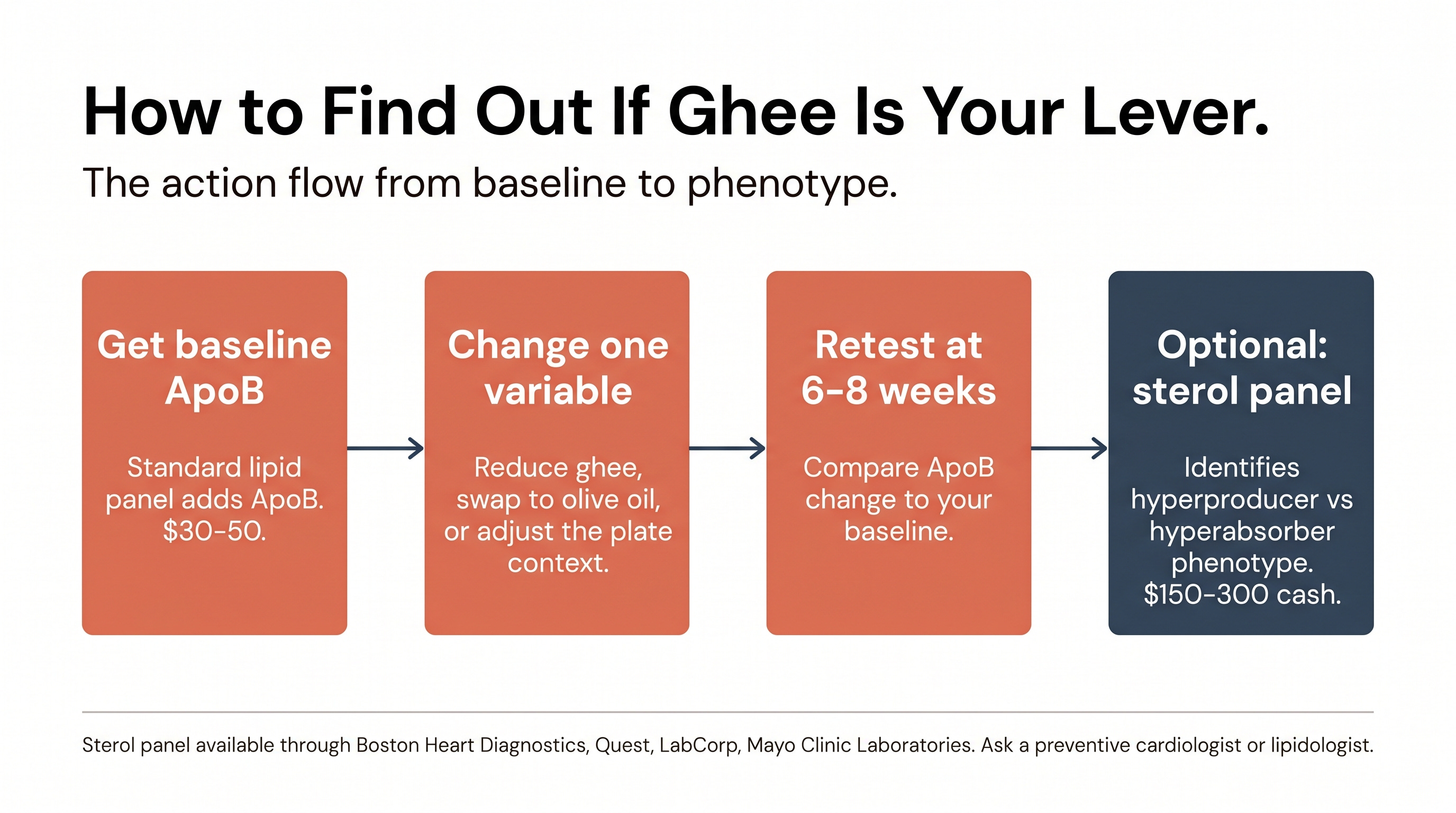
Start with a baseline lipid panel that includes ApoB. Make your dietary change (whether that’s reducing ghee, swapping to olive oil, or adjusting the context around the fat). Retest in 6-8 weeks. One test, one change, your own answer.
If you want to go a level deeper, ask your physician for a sterol panel. It identifies whether you’re a hyperproducer or hyperabsorber, which determines whether dietary fat is a meaningful lever for you at all. Most primary care physicians don’t order these routinely. Ask a preventive cardiologist or lipidologist; Boston Heart Diagnostics, Quest, LabCorp, and Mayo Clinic Laboratories all offer versions, typically $150-300 cash since insurance rarely covers it.
- Dr. Karan Bhalla
The ghee question doesn’t have a universal answer, and that’s what makes it useful. What it does to your numbers depends on your plate, your phenotype, and your labs. The cultural debate becomes a personal one, and the personal one is the one you can act on. Between the auntie, the cardiologist, and the American wife who calls it a superfood, there’s another voice worth listening to: your own data.
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.
Right on the money Karan and Neil. This needs to be talked about more to create awareness in the Indian community.
A simple fat/sterol panel should be made non-negotiable for Indian community, so that hyperabsobers will be cautious. Further, use of Olive or HOSO may be promoted to increase MUFA consumption overall. Mustard is good with ALA, but conversion to EPA (DHA virtually 0) plummet due to Omega-6 competition with desaturases.