
Our Biology Sets a Different Baseline
And why we're starting Desi Vitals


I was diagnosed with fatty liver disease at thirteen and became obese shortly after. I’ve been battling obesity and metabolic disease since then. I’ve gained weight, lost weight, gained it back, and watched doctors shrug at my liver enzymes. It wasn’t until I started tracking my own blood work, body composition, and genetics that I realized how much the standard playbook was missing.
Then my family made it personal. My dad had a heart attack at 69. The angiography revealed 90% blockage in three arteries and 60-70% in three others. His cholesterol was “normal.” His blood sugar was fine. A few years later, my mom’s cousin collapsed at the breakfast table after a morning run, mid-50s, never drank, never smoked, healthy weight. He died before the ambulance arrived. A few months ago, another family member, seemingly in good health, passed away in his car while driving to the hospital.
One in ten heart attacks in South Asian men happens before age 40, roughly 2-3x the rate in Western Europeans (Lancet, 2004; INTERHEART, n=27,000+). Not 60 or even 50, but forty. Dr. Namratha Kandula, who leads the MASALA study on South Asian heart disease, put it simply: “Everyone knows somebody who has had a heart attack at a young age. It’s very common.”
I started paying attention.
TL;DR
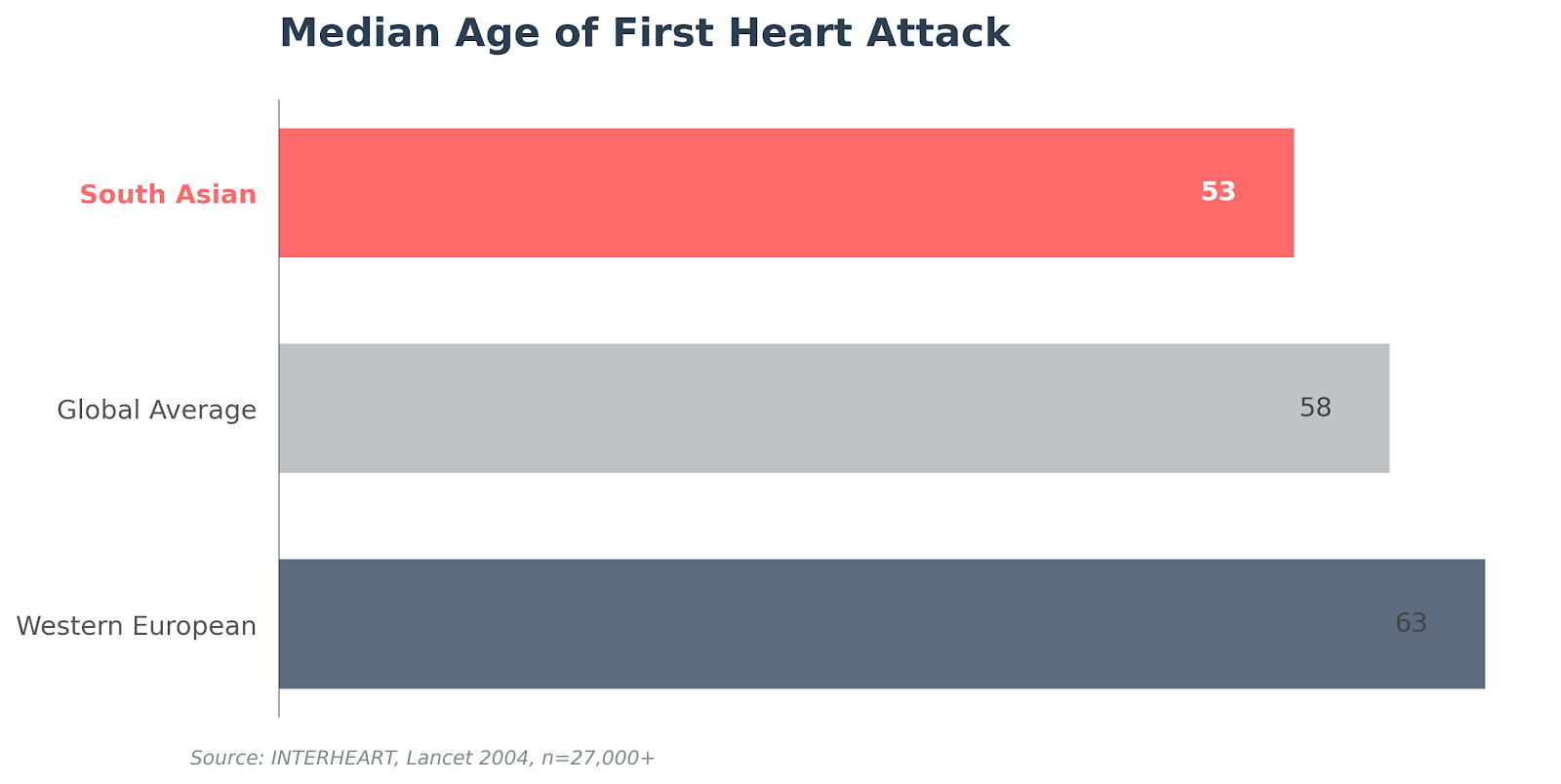
South Asians experience heart attacks 10 years earlier than other populations (median first heart attack: age 53 vs. 63)
Risk factors like prediabetes appear 8x more often by age 45 in South Asian men, even with healthier lifestyles
A CAC scan at 35-40 can show whether plaque has started building, years before symptoms
Standard risk calculators weren’t built for you. Ask for A1c, ApoB, Lp(a), and imaging.
A decade earlier, and lifestyle alone doesn’t explain it
The INTERHEART study found that the median age of first heart attack in South Asians was 53 years, compared to 63 in Western Europe and China (Lancet, 2004; case-control, n=27,000+). A full decade earlier. And 9.7% of South Asian men had their first heart attack before age 40, roughly 2-3x the rate in Western Europeans.
The MASALA study tracked South Asian Americans head-to-head against other ethnic groups and found that despite better diet quality, lower alcohol consumption, and comparable exercise levels, South Asians still carried dramatically higher cardiovascular risk (JAHA, 2026; MASALA/MESA cohort comparison, n=2,700).
South Asian men at age 45 were nearly 8x more likely to have prediabetes than White peers (30.7% vs. 3.9%), with metabolic risk factors appearing at significantly younger ages. The lifestyle was fine, but the biology underneath it wasn’t.
The ruler was built for a different population
At the same BMI, South Asians carry significantly more fat in the places that matter most: visceral fat wrapped around organs, fat deposited inside liver tissue, and fat threaded between muscles (International Journal of Obesity, 2016; MASALA/MESA cross-sectional, n=906). You can look lean and still have a fatty liver driving insulin resistance, and standard BMI cutoffs won’t flag it.
Your cholesterol panel is probably incomplete too. South Asians tend toward a pattern of high triglycerides, low HDL, and small dense LDL particles, what cardiologists call atherogenic dyslipidemia. North Indians develop coronary artery disease at total cholesterol around 170 mg/dL (Indian Journal of Medical Research, 2007), a level most doctors would call normal.
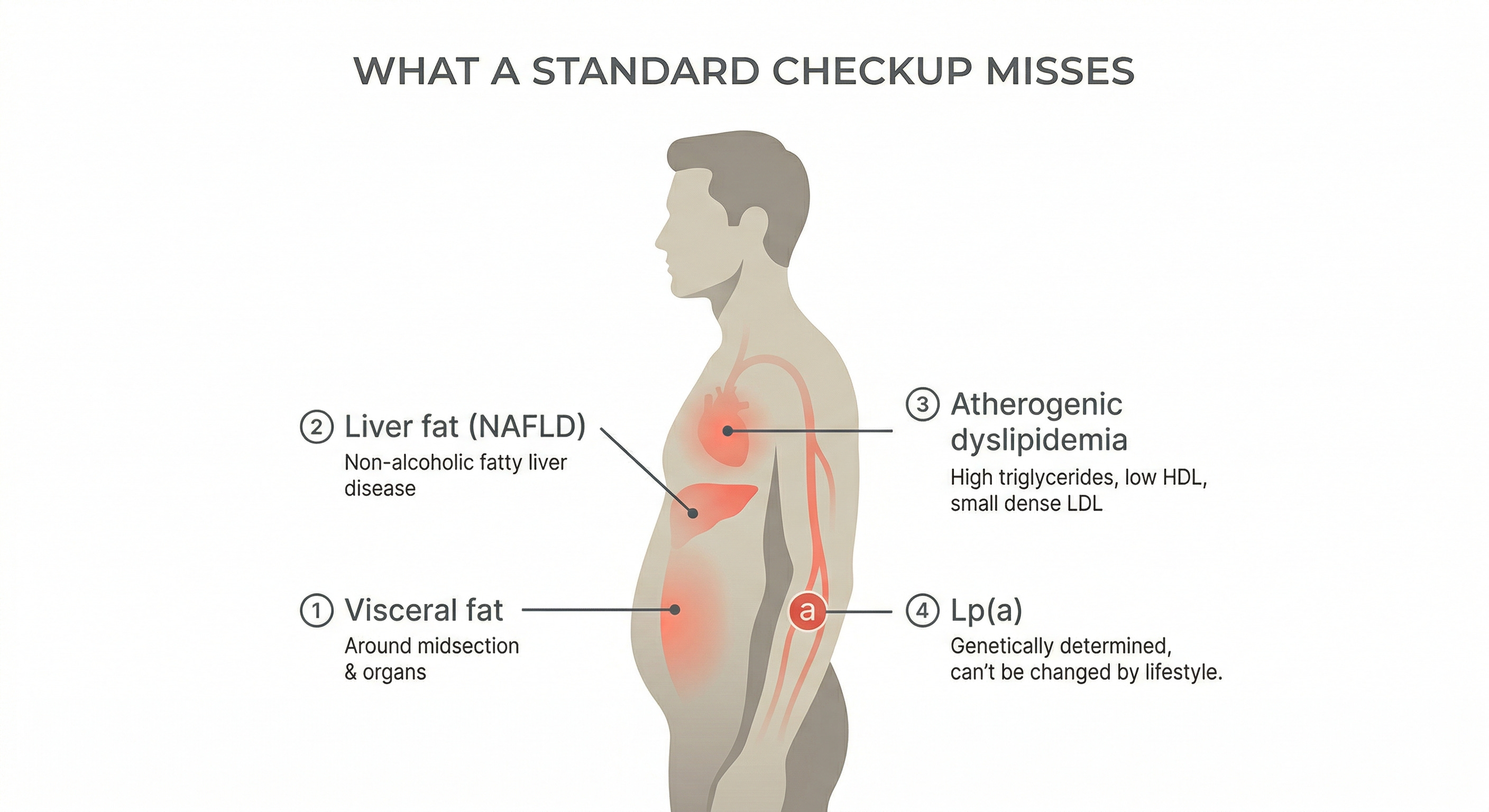
Then there’s Lp(a), a genetically determined cholesterol particle that 25% of South Asians have at elevated levels. It accounts for 9.5% of heart attack risk in South Asians vs. about 4% in White populations (Circulation, 2019; INTERHEART Lp(a) sub-analysis, n=6,086 cases). You can’t diet or exercise it down. The only move is to test it once, know your number, and if it’s high, manage everything else harder.
My ApoB was 103 and nobody blinked
When I finally asked for ApoB, the number that counts every atherogenic particle in your blood, mine came back at 103 mg/dL. My LDL-C at the time was 127 mg/dL, technically flagged high but not a number most doctors would lose sleep over (I know, I was surprised too). Through Zetia, tirzepatide, and psyllium husk, my ApoB is now 83 mg/dL and my LDL-C is 74 mg/dL.
In November 2024, I got a Cleerly CCTA, a coronary CT angiogram that maps plaque in your arteries. It showed my arteries are clean, and my CAC score came back at 0. Reassuring, but not permanent. I’ll repeat it in 3-5 years.
The numbers being good now isn’t the point. Nobody would have caught the problem if I hadn’t asked for the right tests, and I only knew to ask because I went looking.
Good studies, done on different populations
INTERHEART is a case-control study, not a prospective trial, so the 53 vs. 63 comparison has design limitations. The “one in ten before age 40” data is from the global INTERHEART study and may not map perfectly onto diaspora South Asians, though the MASALA study shows similar patterns in South Asian Americans.
Even after accounting for ectopic fat, lipids, and Lp(a), researchers found these factors don’t completely explain the elevated coronary calcium in South Asians (JAHA, 2017; MASALA sub-study, n=803). Something else is contributing, and the theories are still being debated. One possibility: generations of calorie scarcity shaped a metabolism that stores energy efficiently, now mismatched with modern abundance. A 2024 study found that South Asian men who gained weight lost 38% of their insulin sensitivity vs. 7% for European men gaining the same amount (Nature Metabolism, 2024; controlled overfeeding study, n=35). Another thread points to epigenetic inheritance, though this evidence is suggestive rather than conclusive.
The data doesn’t wait for the explanation. Only 3.16% of participants across 310 cardiovascular clinical trials were South Asian (JACC: Asia, 2025; systematic review, n=1M+). The treatment guidelines your doctor follows were largely built on data from other populations.
Myth: “If I eat right and exercise, I should be fine”
The Myth: Heart disease is a lifestyle problem. Maintain a healthy diet, stay active, don’t smoke or drink, and your cardiovascular risk is low.
The Evidence: The MASALA study found that South Asians with better diets and lower alcohol intake still carried dramatically worse cardiovascular risk than other ethnic groups. Munaf Patel is the human version of that data point. He had his first heart attack at 39. He changed everything afterward: diet, exercise, stress management. Eight months later, he had a second heart attack. His father died of heart disease in his 40s (Chicago Tribune, 2019).
Lifestyle absolutely matters, and it’s the first thing any cardiologist will recommend. But for South Asians, lifestyle alone isn’t enough. Our biology works against us in ways that diet and exercise can’t fully offset: excess visceral and liver fat at the same BMI, Lp(a) levels you inherited and can’t change, and an atherogenic lipid pattern that a standard panel doesn’t even measure.
The Verdict: Lifestyle matters, but for South Asians, biology sets a different baseline.
There’s no shortage of health content out there: newsletters, podcasts, longevity influencers. But almost none of it is written for the South Asian body. The dietary advice assumes a Western diet. The risk calculators were calibrated on European populations. The clinical trials enrolled almost no South Asians. And most of our community has no idea how different our risk profile actually is.
I’m writing Desi Vitals with my dear friend Dr. Karan Bhalla. Karan is a board-certified interventional cardiologist in Houston, Texas. He trained at Seth G.S. Medical College in Mumbai, did his cardiology and interventional fellowships at UTHealth McGovern, and co-founded Orion Medical, where he’s been practicing for over fifteen years. He’s a Fellow of the American College of Cardiology, past president of the Harris County Medical Society, and faculty at McGovern Medical School. He sees South Asian patients with exactly these risk patterns every day. I bring the patient side, Karan brings the clinical side, and together we aim to do the work of reading the research, talking to the experts, and synthesizing it into clear, actionable information so you don’t have to spend hours sorting through scientific papers and podcasts to figure it out yourself.
Desi Vitals is the newsletter we wish had existed when we first started paying attention. Evidence-based South Asian cardiometabolic health, written for our community, by people who’ve lived it.