
The Fasting Insulin Number Nobody Orders
The $30 test that catches metabolic dysfunction a decade before glucose moves


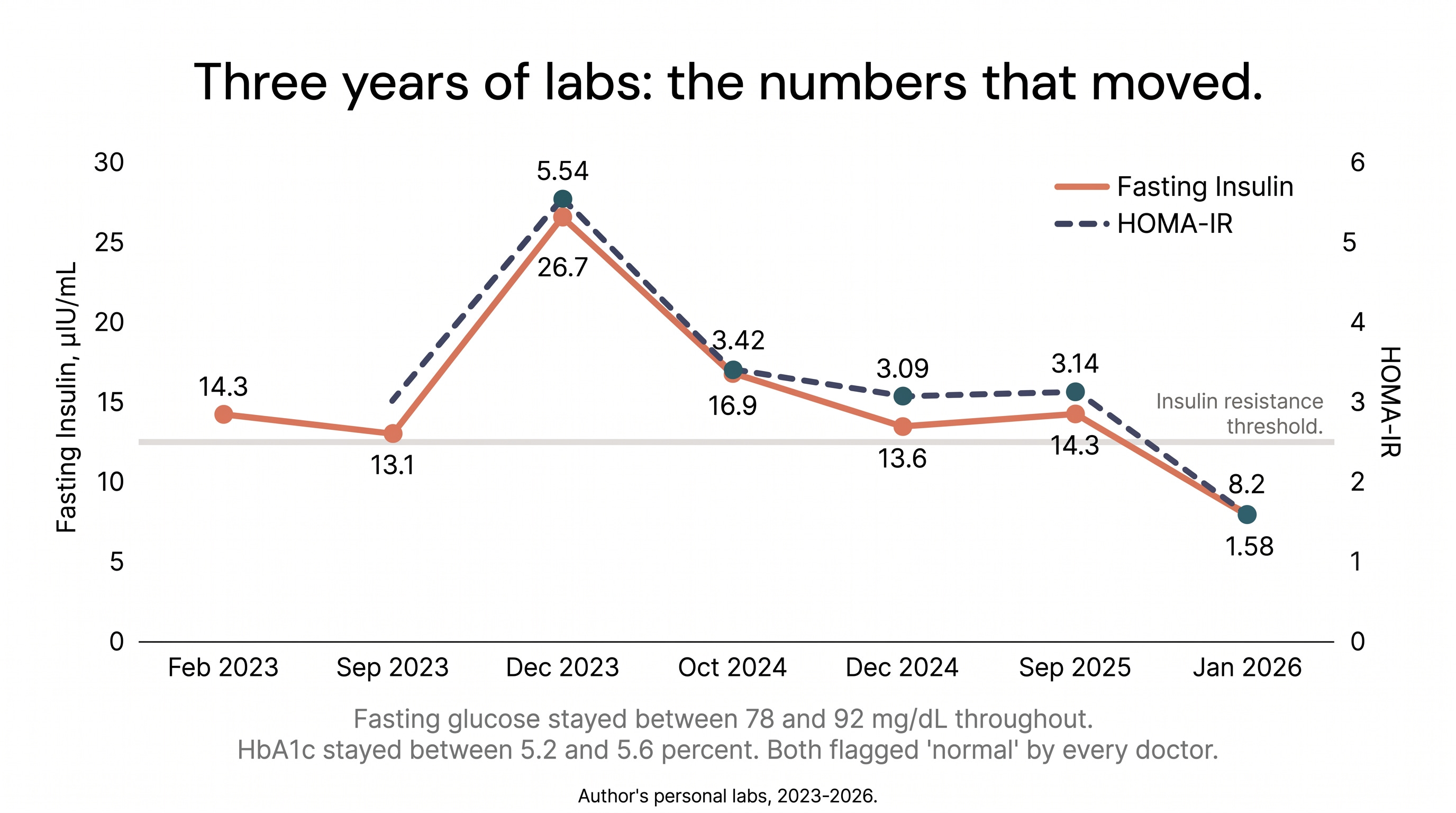
In December 2023, my fasting insulin came back at 26.7 µIU/mL, 45% above the upper reference limit. My glucose was 84. My HbA1c was 5.6%. Both “normal.” Every standard screening marker said I was fine.
When I calculated my HOMA-IR, a single score that quantifies insulin resistance, it came out to 5.54. Anything above 2.5 means insulin resistant. I was more than double that threshold, and no doctor flagged it.
That number connected directly to the fatty liver disease I’d had since age thirteen. Insulin resistance was driving the fat accumulation the whole time, and fasting insulin would have shown it years earlier than anything else in my labs. In our diagnostics post, we listed fasting insulin as one of the core markers. This is why.
The Bottom Line
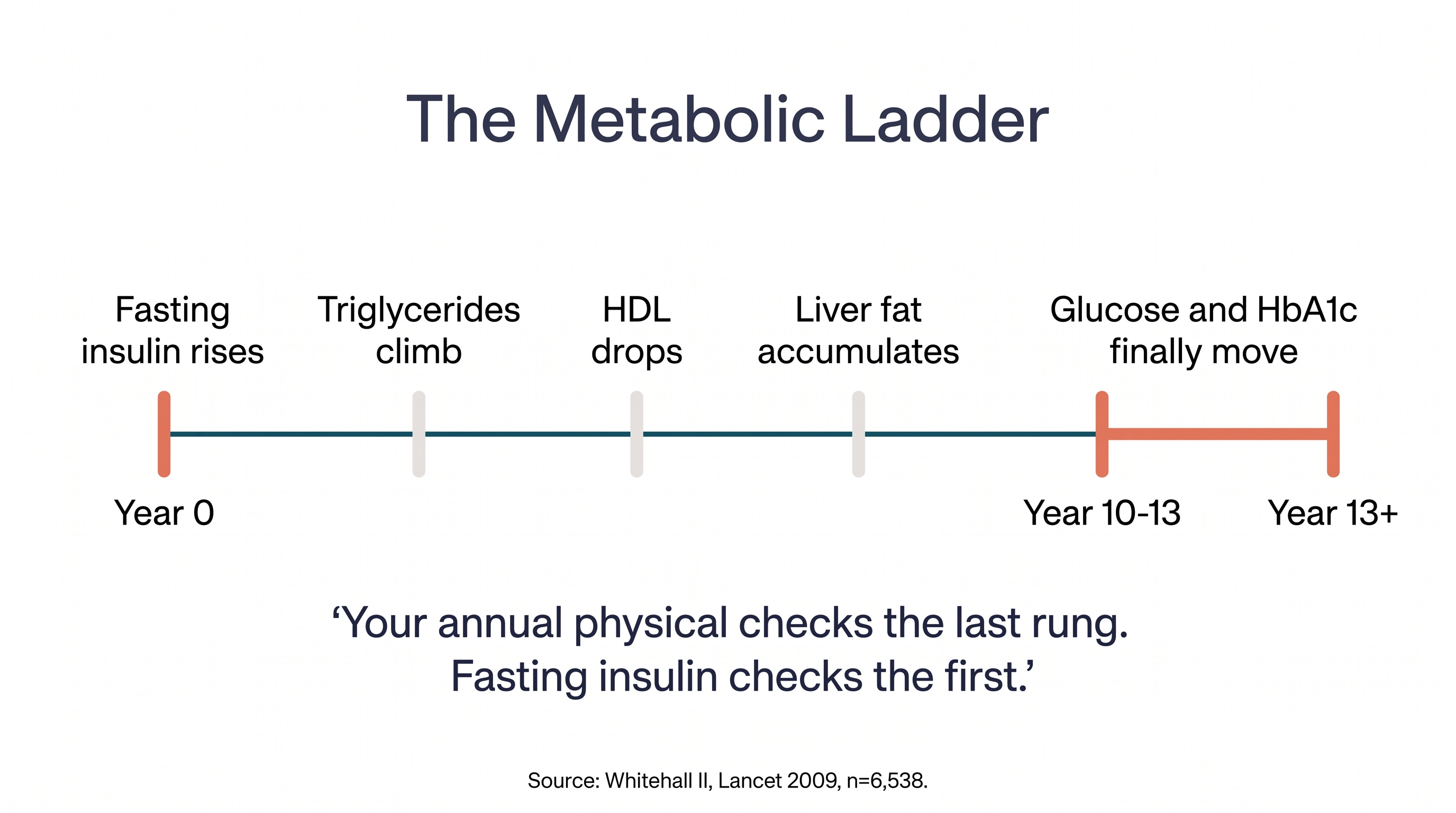
Fasting insulin rises 10-13 years before glucose or HbA1c becomes abnormal (Lancet, 2009; Whitehall II, n=6,538)
75% of glucose-normal people have abnormal insulin patterns (Kraft database, n=14,384)
Track four numbers together: fasting insulin, fasting glucose, HbA1c, and HOMA-IR. Any one alone can miss what the others catch. HOMA-IR = (insulin x glucose) / 405. Above 2.5 = insulin resistant.
A fasting insulin test costs $20-30. Most doctors don’t order it. Ask.
Your annual physical checks the last rung, not the first
Metabolic dysfunction works like a ladder. Insulin rises first, then triglycerides climb, HDL drops, and your liver starts storing fat. Years later, glucose and HbA1c finally move. Your annual physical checks the last rung. Fasting insulin checks the first.
The Whitehall II study tracked over 6,500 people for 13 years and found that future diabetics already had significantly lower insulin sensitivity 13 years before diagnosis (Lancet, 2009; prospective cohort, n=6,538). Glucose only spiked in the final 2-3 years. The body compensates for insulin resistance by pumping out more insulin, keeping glucose in range, until it can’t. Standard screening catches the final stage: when compensation fails and glucose finally spikes.
That’s where HOMA-IR comes in. It turns two numbers from a standard blood draw into one insulin resistance score: below 1.0 is optimal, above 2.5 is insulin resistant, and above 5.0 is severe. The formula is simple: (fasting insulin x fasting glucose) / 405. You can calculate it yourself from any lab that includes both numbers.
Why doesn’t your doctor order fasting insulin? Because it’s not in the ADA screening guidelines. The entire diabetes screening paradigm is built around glucose, which is the last thing to break, not the first. The test exists and costs $20-30. The guidelines just haven’t caught up.
The “normal” range is lying to you
The reference range on your lab report makes this worse. Most labs call anything between 2 and 18.4 µIU/mL normal, but a fasting insulin above 9.0 already identifies prediabetes in 80% of affected patients (Endocrine Practice, 2009; cross-sectional, n=2,000+). At 14.3 µIU/mL, my lab report said normal. I was already well into insulin resistance territory by functional standards.
For South Asians, the standard ranges are even more misleading. HOMA-IR values run 67% above European averages (Diabetologia, 2013; Ghouri et al., age- and BMI-matched, n=186). When both groups gained the same weight, South Asians lost insulin sensitivity at roughly five times the rate: a 38% decrease compared to 7% in white Europeans (Nature Metabolism, 2024; GlasVEGAS controlled feeding study, n=35). The margin for early detection is thinner, the consequences arrive sooner, and the standard cutoffs were built on a different population.
I’m obese, and my glucose said I was fine
I’ve been obese since childhood. I was diagnosed with fatty liver disease at thirteen. By any common-sense measure, something is clearly off metabolically. But look at the glucose and A1c columns below.
Date Insulin (µIU/mL) Glucose (mg/dL) HbA1c (%) HOMA-IR Feb 2023 14.3 - 5.3 - Sep 2023 13.1 - 5.2 - Dec 2023 26.7 84 5.6 5.54 Oct 2024 16.9 82 5.4 3.42 Dec 2024 13.6 92 5.2 3.09 Sep 2025 14.3 89 - 3.14 Jan 2026 8.2 78 5.2 1.58
Glucose never left the normal range. HbA1c barely moved. If you only looked at the standard panel, you’d say I was metabolically healthy. Meanwhile, fasting insulin was screaming. At its peak, my HOMA-IR hit 5.54, more than double the threshold for insulin resistance, and not a single doctor flagged it.
The numbers that caught the problem were the ones nobody ordered: fasting insulin and HOMA-IR. That’s how the test is designed.
What HOMA-IR can and can’t tell you
HOMA-IR is a fasting-only measure. It tells you nothing about what happens after a meal. Someone can have a normal HOMA-IR and still have terrible post-meal glucose spikes, which is what a CGM can reveal. The two work together: HOMA-IR catches the baseline, a CGM catches the response.
One caveat on the numbers themselves: if you get your insulin tested at two different labs, you might get two different results. The tests aren’t perfectly standardized yet. That’s fine. What matters is the trend over time at the same lab, not any single number. Pick a lab and stick with it.
An elevated HOMA-IR is a conversation with your doctor, not a self-diagnosis. It’s a screening tool that opens a door. I’m watching whether mine holds below 2.0 as I continue to lose weight.
Myth: “My glucose is normal, so I’m metabolically healthy”
The Myth: Your annual physical checks fasting glucose or HbA1c. If those numbers are normal, your metabolism is working fine. You’d know if something was wrong.
The Evidence: The Kraft database, validated across 14,384 patients with extended glucose-insulin tolerance tests, found that 75% of people with normal glucose had abnormal insulin patterns (Crofts et al., Diabetes Research and Clinical Practice, 2015; n=14,384). A study of 1,313 young adults in Mumbai found 30.5% had hyperinsulinemia with completely normal glucose, and among those with HbA1c below 5.7%, nearly 40% had stimulated insulin above 80 mIU/mL (Frontiers in Clinical Diabetes, 2023; n=1,313). Globally, 1 in 4 adults has insulin resistance (Frontiers in Endocrinology, 2025; meta-analysis, n=235,148). Most don’t know it because the test that catches it isn’t part of standard screening.
The Verdict: Normal glucose is the last domino to fall, not the first sign that everything is fine.
One Thing I Changed
I now test my fasting insulin in my quarterly draws, and track that along with HOMA-IR so I can get a better sense of my metabolic health over time.
Add fasting insulin to your next blood draw
At your next visit, ask your doctor to add fasting insulin to your metabolic panel. It’s a $20-30 add-on. Together with fasting glucose, HbA1c, and HOMA-IR (which you can calculate yourself), these four numbers catch insulin resistance years before any one of them would alone. For my South Asian patients, I consider a Fasting Insulin above 10, and HOMA-IR above 2.5 a red flag that changes the conversation about diet, exercise, and potentially medication. Track all four over time at the same lab. The trend is the signal.
-Dr. Karan Bhalla
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.