
The Liver Is a Metabolic Amplifier
One in three South Asians has fatty liver. It sits at the center of a metabolic loop.


When I was diagnosed with fatty liver disease at thirteen, the doctor said one thing: lose weight. For the next 25 years, that was the only advice I ever got.
My ALT was always elevated, and every doctor shrugged and repeated the same line. Nobody mentioned my heart. Nobody mentioned that my liver was both a symptom and an accelerator of a metabolic problem building across multiple organ systems.
It turns out that fatty liver, now called MASLD (metabolic dysfunction-associated steatotic liver disease), sits at the center of a metabolic cascade that connects to cardiovascular disease, Type 2 diabetes, and kidney disease.
The Bottom Line
Fatty liver is now MASLD: renamed in 2023 to reflect that it’s a metabolic condition, not a drinking problem
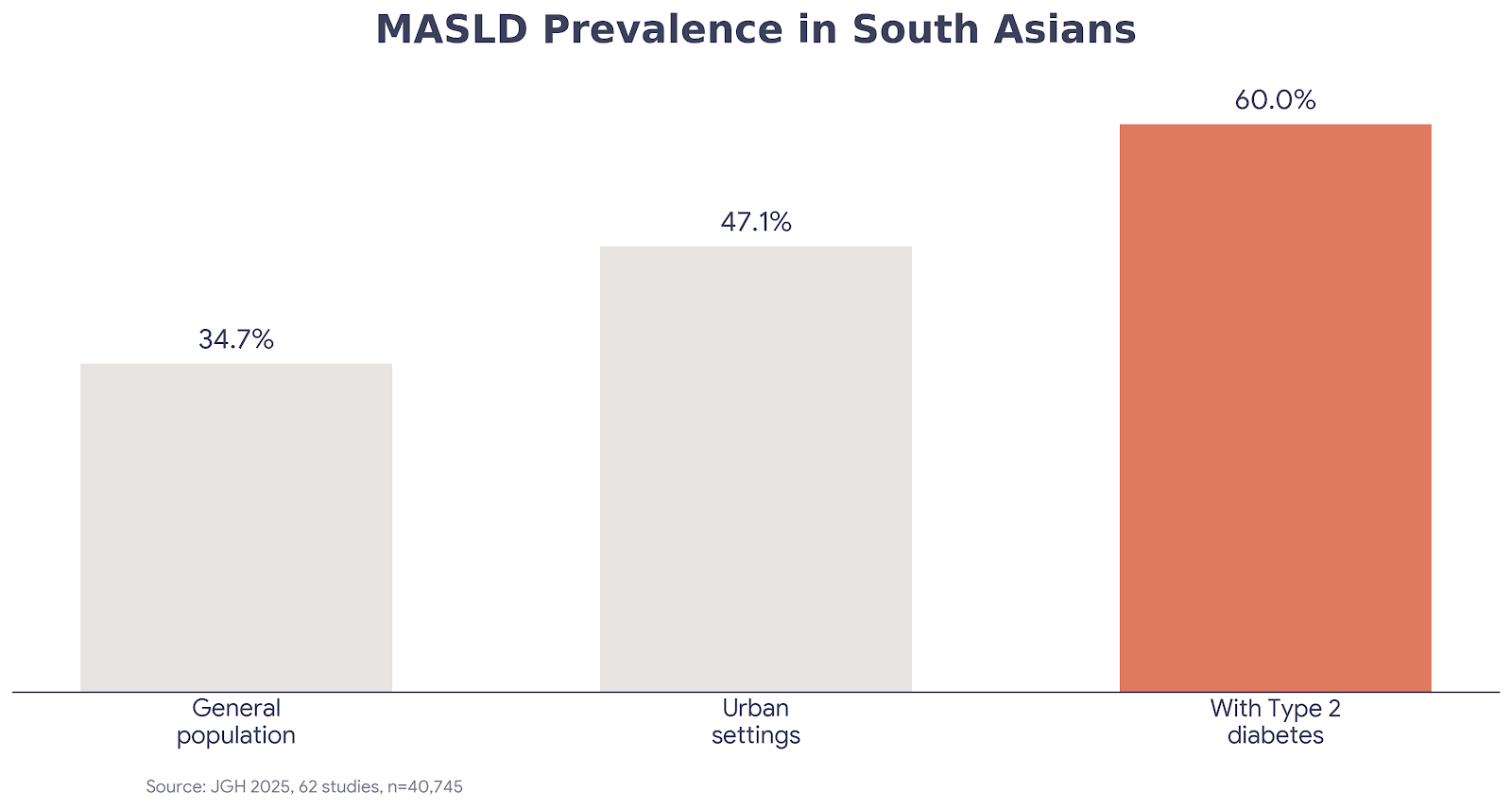
34.7% of South Asians have MASLD, with rates as high as 48% at BMI ≥25 (JGH, 2025; 62 studies, n=40,745)
MASLD and heart disease share the same metabolic root: insulin resistance. The liver amplifies the signal, with significantly higher cardiovascular risk even after adjusting for other metabolic factors
Standard liver enzymes (ALT/AST) are normal in ~25% of patients with significant fatty liver
One in three South Asians has it, and most don’t know
The largest meta-analysis of MASLD in South Asians pulled 62 studies covering 40,745 people and found a prevalence of 34.7% in the general population, rising to 60% among those with Type 2 diabetes (Journal of Gastroenterology and Hepatology, 2025; systematic review and meta-analysis, n=40,745). The mean BMI of those South Asian patients was only 24.8, barely above the normal range.
Globally, about 19% of normal-weight individuals have MASLD, and lean MASLD is more prevalent in Asia than anywhere else. A mean BMI of 24.8 means many of these patients wouldn’t trigger screening under standard Western guidelines. You can be at a weight most doctors would call healthy and still have fat accumulating in your liver.
The fibrosis data is what concerned me most. South Asian MASLD patients had advanced fibrosis (scarring) at a rate of 14%, roughly double the rates found in European and American cohorts (JGH, 2025). Lower BMI, higher fibrosis rates, worse outcomes at every stage.
The liver is a metabolic amplifier
For years I thought of my fatty liver as a liver problem. It’s actually a signal that the entire metabolic system is under stress, and the liver both reflects that stress and makes it worse.
The mechanism works through insulin resistance, the common root. When the liver accumulates fat, it becomes less responsive to insulin, which drives dangerous cholesterol patterns (more small dense LDL, higher triglycerides, lower HDL), chronic inflammation, and elevated blood sugar. Those same pathways drive cardiovascular disease and diabetes independently. The liver sits in the middle, amplifying all of it.
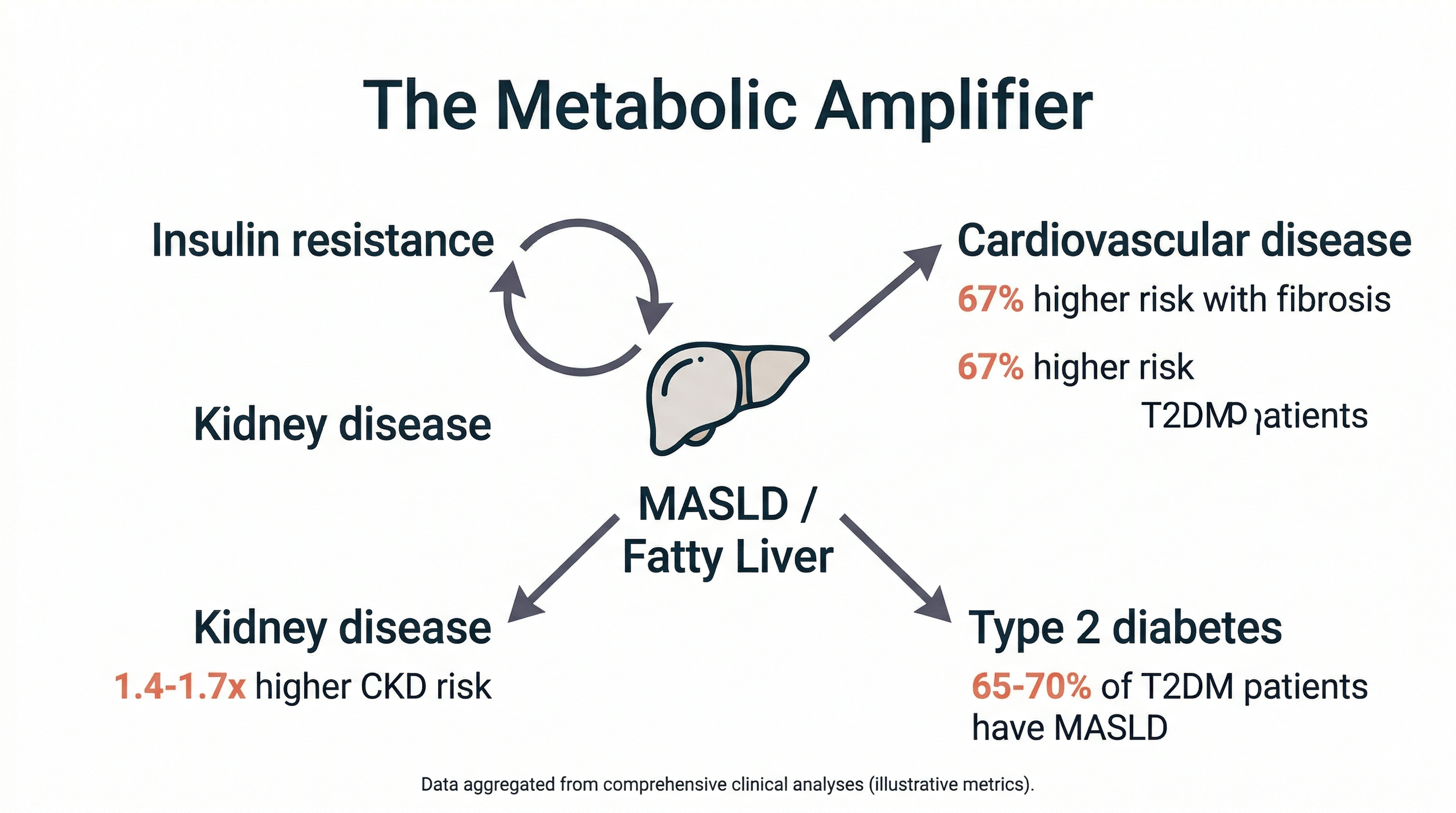
A nationwide Swedish cohort study (n=10,422) found that MASLD patients had 67% higher cardiovascular risk with noncirrhotic fibrosis and 115% higher with cirrhosis, even after accounting for traditional cardiometabolic risk factors. But most of the excess risk comes from the shared metabolic drivers (insulin resistance, inflammation, visceral fat), not from the liver itself. The liver is an accelerator, not the root cause.
The connection to diabetes runs both directions. Up to 65-70% of people with Type 2 diabetes have MASLD, and 15-30% of MASLD patients develop Type 2 diabetes within five years. In the South Asian meta-analysis, prevalence among T2DM patients was 60% (JGH, 2025). South Asians already have 1.5-2x higher insulin resistance at the same BMI as European populations.
“I see patients with clean lipid panels and normal-looking physicals who have significant fatty liver on imaging. The standard cardiac workup doesn’t include liver assessment, and the standard liver workup doesn’t include cardiac risk. MASLD falls in the gap between the two specialties, and South Asian patients are the ones most likely to be sitting in that gap.”
- Dr. Karan Bhalla
Your ALT might be lying to you
Two problems make MASLD harder to catch than it should be. First, approximately 25% of MASLD patients have completely normal ALT and AST levels (BMC Gastroenterology, 2020; meta-analysis, 11 studies, n=4,084). Many patients are asymptomatic with liver function tests that look fine. A normal ALT does not mean a healthy liver.
Second, the diagnostic criteria were redesigned in 2023 when NAFLD was renamed MASLD. The new criteria use a BMI threshold of 23 for Asian populations, not 25 (which, if you’re South Asian, probably applies to you or someone in your family). That single number means South Asians qualify for screening at a lower weight than other groups, but most primary care doctors are still using the old cutoffs.
The practical starting point is a FIB-4 score, which uses four numbers from a standard blood panel (age, ALT, AST, platelets) to estimate fibrosis risk with no extra blood draw. If you’ve had a DEXA scan, check your visceral adipose tissue number: elevated visceral fat is strongly associated with liver fat, and you may already have that data sitting in a report. FibroScan is the next step if staging is needed, but start with what’s accessible.
28 years and counting
My ALT has been elevated for 28 years, and the January 2026 result of 84 U/L is still nearly double the upper limit.
But my DEXA scans tell a clearer story than my liver enzymes. Visceral fat dropped from 5.5 to 3.89 lbs over the past year, and my CCTA (coronary CT angiography) in November 2024 showed zero coronary atherosclerosis despite 28 years of NAFLD. DEXA and CCTA track progress that liver enzymes miss. If I had relied on ALT alone, I would have assumed nothing was changing.
I’m on tirzepatide, a GLP-1/GIP dual agonist. GLP-1 receptor agonists significantly reduce liver fat (some studies suggest reductions of up to almost 50%) (Wang et al., 2025; systematic review, 25 RCTs, n=2,600). For a condition that had zero approved treatments for decades, there are now three on the table (resmetirom, semaglutide for MASH, and tirzepatide showing the highest efficacy in late-stage trials).
What the data can’t tell us yet
The 2025 South Asian meta-analysis has very high heterogeneity, with prevalence ranging from 18.5% in rural settings to 47.1% in urban ones. Detection method matters enormously, and these numbers will sharpen as more studies use standardized MASLD criteria.
The Mendelian randomization evidence on CVD causality is nuanced: genetic variants that cause liver fat (PNPLA3, TM6SF2) show weak or no causal link to heart attacks, suggesting that the liver fat itself isn’t the direct CVD driver. The inflammatory pathways that come with it likely are. The clinical implication is that treating the metabolic dysfunction (insulin resistance, inflammation, visceral fat) matters more than treating the liver in isolation.
Most MASLD is driven by insulin resistance and caloric excess. Genetic factors like choline metabolism can play a role (they do in my case), but they’re one pathway among many.
Myth: “Fatty liver is caused by drinking too much”
The Myth: Fatty liver disease is a consequence of heavy alcohol use. If you don’t drink, or barely drink, you don’t need to worry about it.
The Evidence: MASLD (metabolic, non-alcohol-related fatty liver disease) now affects 38% of all adults globally, up from 25% two decades ago (Hepatology, 2024; 92-study meta-analysis). It is more common than alcohol-related liver disease worldwide. The primary driver is insulin resistance and metabolic dysfunction, not alcohol. The 2023 renaming from NAFLD to MASLD explicitly addressed this confusion: the old name implied that the default fatty liver was alcoholic. The new name drops the alcohol framing entirely and centers cardiometabolic risk. Many of the South Asian patients in the meta-analysis had a BMI that most doctors wouldn’t flag, and many have never had a drink.
The Verdict: Busted. MASLD is a metabolic condition, not a drinking problem. Insulin resistance, visceral fat, and metabolic dysfunction are the primary drivers.
One Thing I Changed
I added a gut-liver axis probiotic to my morning routine, targeting the connection between gut barrier function and liver inflammation (this took me a surprisingly deep research rabbit hole to land on a specific strain). Too early for results, but I’m tracking ALT at my next draw.
Twenty-eight years with this condition, and I’m only now understanding the full picture of what it connects to. The liver, the heart, blood sugar, kidney function: they’re all part of the same metabolic story.
Fatty liver screening beyond ALT
Ask your doctor to calculate your FIB-4 score from your existing labs. It uses age, ALT, AST, and platelets to estimate liver fibrosis risk, and no new blood draw is needed. If you’ve had a DEXA scan, check your visceral adipose tissue number: elevated VAT is one of the strongest signals for fatty liver, and you may already have the data. For my South Asian patients, I use the MASLD diagnostic criteria starting at BMI 23, not 25. One calculation, one conversation.
- Dr. Karan Bhalla
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.