
The Non-Statin LDL Toolkit
Four FDA-approved drug classes with real outcome data, plus one soluble fiber that belongs in the conversation.


When I tell people I managed my LDL and ApoB for years without a statin, the most common reaction is: “Wait, you can do that?”
I stopped rosuvastatin because the metabolic cost was too high for someone already managing metabolic syndrome (covered in Part 1). Other people stop for muscle pain. Many never start because they’ve heard statins cause dementia, a worry the data doesn’t support: meta-analyses of randomized trials show no impact on cognition or dementia risk, and large observational studies have found a small reduction in dementia risk among statin users (Ott et al., Journal of General Internal Medicine, 2015; meta-analysis of RCTs).
For a while, I assumed my options were limited. They weren’t. Four FDA-approved drug classes now have cardiovascular outcome data, meaning they’ve been proven to prevent heart attacks and strokes, not just lower a number on a lab report. Most people who stop or avoid statins never hear about them. And one humble soluble fiber has real LDL-lowering evidence that slots in alongside these drug classes.
If you stopped a statin and haven’t replaced it with anything, you’re not alone. The “statins or nothing” framing is years out of date. Here’s what actually exists.
The Bottom Line
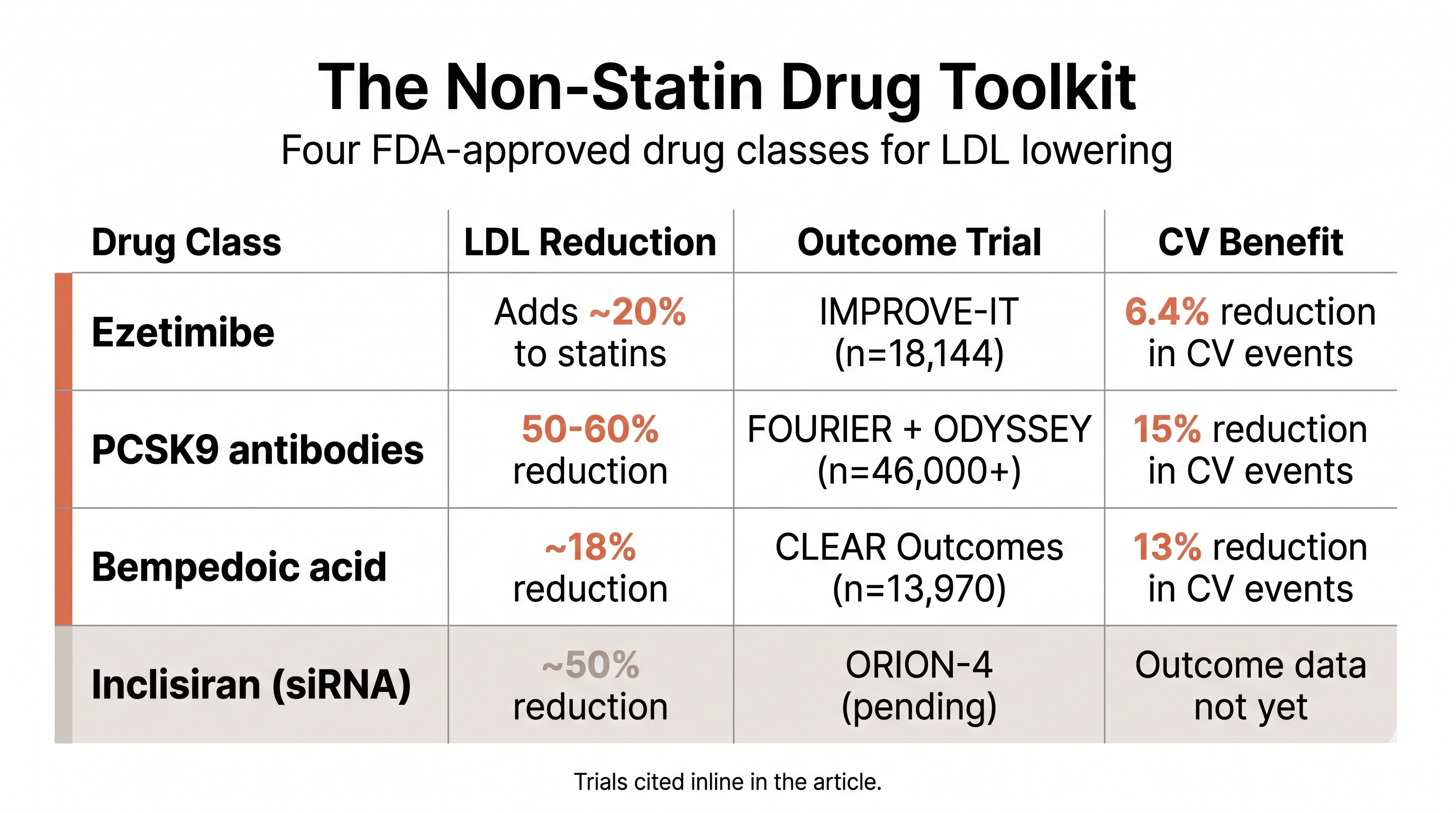
Four non-statin drug classes now have cardiovascular outcome data: ezetimibe, PCSK9 inhibitors, bempedoic acid, and (partially) inclisiran
Moderate statin + ezetimibe achieves similar LDL targets with 18% less diabetes risk than high-intensity statin alone
PCSK9 inhibitors are now as low as $25/month with insurance
Psyllium husk is the one non-drug adjunct with real LDL and ApoB data. Covered in Part 2 of this series.
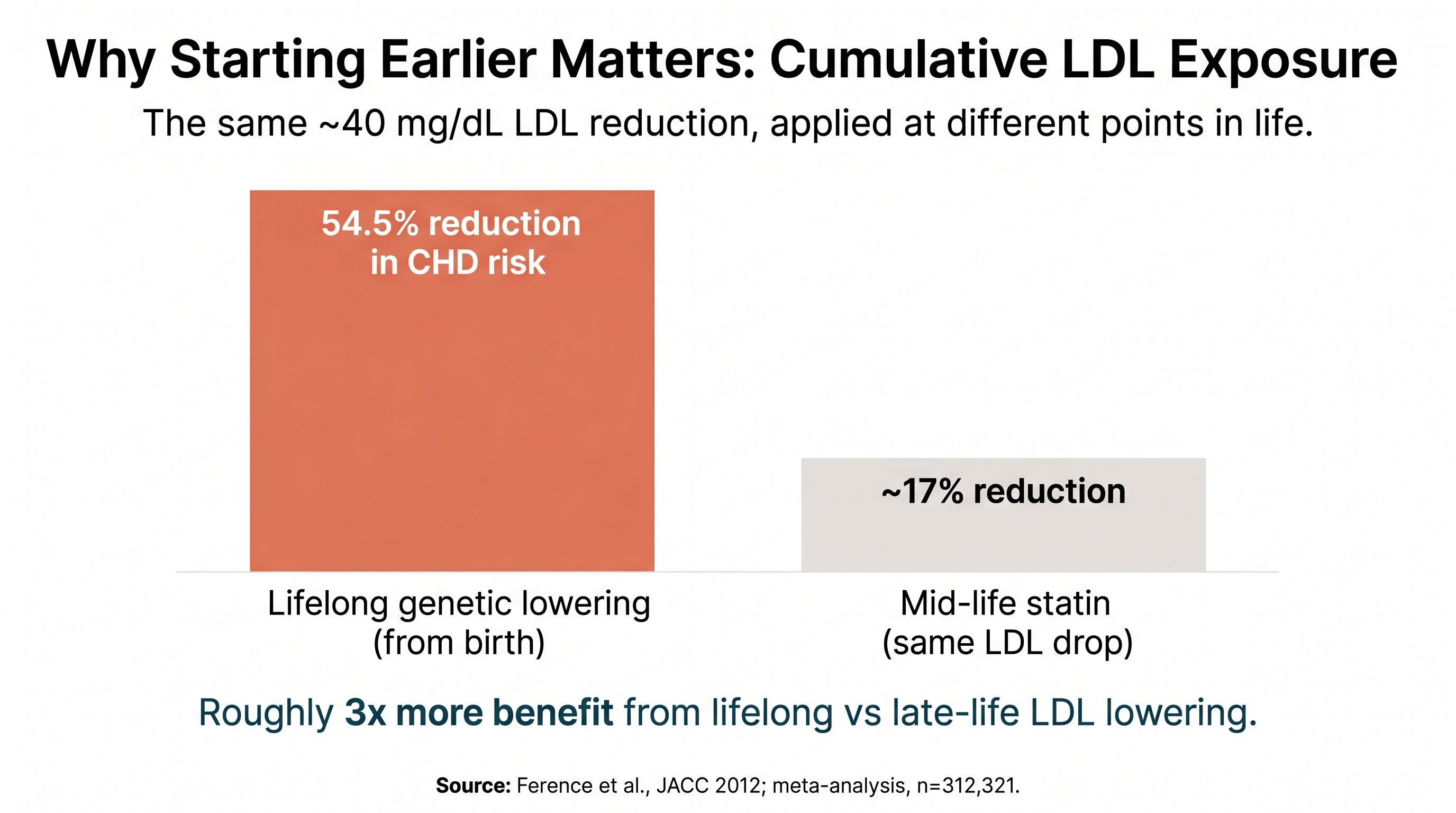
Every year of delayed LDL lowering compounds plaque buildup. Mendelian data shows roughly 3x more benefit from lifelong versus late-life lowering.
A $10 generic that made outcome trials boring
Ezetimibe (sold as Zetia) is the most accessible non-statin option and probably the most underappreciated. It blocks cholesterol absorption in the intestine through a different pathway than statins, so the effects are additive when combined.
IMPROVE-IT (NEJM, 2015; RCT, n=18,144) tested ezetimibe added to simvastatin in post-heart-attack patients. The result: a 6.4% relative reduction in the primary composite endpoint. That’s a real but modest benefit, which is why it never made headlines. The diabetes profile is what makes ezetimibe interesting for this audience. A pooled analysis of 4 cohort studies found that moderate statin + ezetimibe achieved similar LDL targets with 18% less new-onset diabetes than high-intensity statin monotherapy. Same destination, different metabolic cost.
Generic ezetimibe costs roughly $10/month. For someone concerned about statin side effects or diabetes risk, moderate statin + ezetimibe may be the smarter combination. Ezetimibe alone (about 18-20% LDL reduction as monotherapy) is also a real option for someone fully off statins, though the combination evidence is stronger. Worth asking about.
The injectable that costs less than you think
PCSK9 inhibitors (the antibody versions are sold as Repatha and Praluent) are the most powerful LDL-lowering tools available. They’re monoclonal antibodies that block PCSK9, a protein that normally breaks down LDL receptors on liver cells. Blocking PCSK9 means your liver clears more LDL from your blood, and the therapy is delivered as a subcutaneous injection every two to four weeks depending on dose.
The outcome data is strong. FOURIER (NEJM, 2017; RCT, n=27,564) showed a 15% reduction in the primary cardiovascular endpoint with evolocumab. ODYSSEY Outcomes (NEJM, 2018; RCT, n=18,924) showed a 15% reduction with alirocumab. Combined, that’s over 46,000 patients in landmark trials with hard endpoints. No diabetes signal in either trial, despite massive LDL lowering.
The cost story has changed dramatically. Repatha is available at $239/month through the AmgenNow direct-to-patient program (launched October 2025), roughly 60% below the list price. With some insurance coverage, co-pays can be as low as $25/month. The “$14,000/year” number that scared everyone off was 2015 pricing.
One caveat worth noting: inclisiran works differently from PCSK9 antibodies. It’s a small interfering RNA that silences PCSK9 production at the genetic level, which is why a single injection lasts about six months. The technology is genuinely novel and the side effect profile, in theory, should be minimal. But the cardiovascular outcome data isn’t in yet. ORION-4 (n=~15,000) is the phase 3 outcome trial that will answer whether LDL lowering translates into event reduction. Until that reports, inclisiran belongs in a different evidence category than ezetimibe, PCSK9 antibodies, or bempedoic acid.
Built for people who can’t take statins
Bempedoic acid (sold as Nexletol) is the newest option on this list and the most relevant for statin-intolerant patients. It works on the same cholesterol pathway as statins but upstream, and here’s the key difference: it’s a prodrug that activates only in the liver, not in skeletal muscle. No muscle activation means no myalgia, which is the side effect that sends most people to the supplement aisle in the first place.
CLEAR Outcomes (NEJM, 2023; RCT, n=13,970) was the first trial to show cardiovascular benefit in statin-intolerant patients specifically. The result: 13% reduction in major cardiovascular events. The diabetes profile was favorable, trending protective with no HbA1c or glucose increase. In a prespecified diabetes subgroup analysis, the benefit was even stronger: a 2.4% absolute risk reduction in major cardiovascular events (Lancet Diabetes & Endocrinology, 2024).
For someone who genuinely can’t tolerate any statin, bempedoic acid + ezetimibe is the combination with the strongest evidence base, achieving roughly 38% LDL reduction combined.
One practical wrinkle worth knowing before the appointment: with how insurance approvals work today, it’s now often easier to get a PCSK9 inhibitor covered than bempedoic acid, even for statin-intolerant patients. Coverage favors the drug class with longer and stronger outcome data, even when the newer option fits the clinical profile better. A small access reality that can flip the order of what you actually try first.
The soluble fiber that still earns its place
Before leaving the toolkit, the one non-drug adjunct: psyllium husk, what most South Asian households know as Isabgol. Part 2 of this series covered the evidence in detail (the meta-analysis, the mechanism, the dose, the cost, the cross-link to my deeper write-up). It belongs in any non-statin conversation, and it’s been part of my own regimen.
The statin-intolerant patients who come into my clinic have usually been told ‘try lifestyle changes’ and sent home. That’s incomplete. For somebody with elevated risk, especially South Asian patients where the window is narrower, the right conversation is which non-statin agent or combination to start, and how soon. Ezetimibe plus bempedoic acid is a strong place to begin for someone who can’t take any statin. Adding psyllium on top is cheap and meaningful. A PCSK9 inhibitor enters the picture if the LDL target is still not reached or if the risk profile warrants it.
- Dr. Karan Bhalla
Every year you wait, your arteries remember
The urgency behind all of this comes from one concept: cumulative LDL exposure. Atherosclerosis is driven by the total LDL-years your arteries have experienced, not your LDL level today.
The data on this is striking. People born with genetic variants that naturally lower LDL by roughly 40 mg/dL from birth experience a 54.5% reduction in coronary heart disease risk (Ference et al., JACC, 2012; meta-analysis, n=312,321). That’s roughly three times the benefit seen when a statin delivers the same 40 mg/dL reduction starting in middle age, according to the same analysis. The European Atherosclerosis Society consensus confirms the effect is both causal and cumulative.
For South Asians, with coronary disease onset roughly 10 years earlier than European populations, the window for early treatment is narrower and the cost of delay is steeper. The question has shifted from “statin or nothing” to how soon, by how much, and with which tool.
How low is low enough?
Whatever you settle on, the next question is how aggressively to push the numbers. The 2019 ESC/EAS guidelines, still current as of the 2025 focused update, call for LDL below 55 mg/dL for very-high-risk patients (existing cardiovascular disease, diabetes with target organ damage, familial hypercholesterolemia) and below 40 mg/dL for those with recurrent events on maximum therapy (Mach et al., European Heart Journal, 2019; consensus guidelines). The American ACC/AHA guidelines sit at LDL below 70 mg/dL for similar profiles, moving in the same direction.
ApoB tracks alongside. The widely cited targets: below 80 mg/dL for high-risk and below 65 mg/dL for very-high-risk patients.
For South Asians, where 10-year ASCVD risk is systematically underestimated by standard calculators, the case for hitting the lower end is stronger. Practically: if you have a strong family history of early heart attack, stroke, or diabetes, treat yourself as “high risk” or “very high risk” even without a prior cardiac event of your own. The biology of cumulative LDL exposure is the same; the starting risk isn’t.
What these trials can’t tell us yet
The PCSK9 inhibitor and bempedoic acid trials enrolled predominantly white populations. South Asians are underrepresented in all four major outcome trials covered here. The direction of evidence is strong, but ethnic-specific benefit-risk ratios are estimated, not proven. Inclisiran’s outcome data (ORION-4) is still pending. And the optimal sequencing of non-statin therapies (which to try first, which combinations work best for which risk profiles) is still being worked out in clinical practice. The evidence base is expanding faster than the guidelines.
Myth: “If I can’t tolerate statins, there’s nothing else I can do”
The Myth: Statins are the only proven way to lower LDL and prevent cardiovascular events. If you get side effects, your choice is suffering through them or going unprotected.
The Evidence: The belief persists because of three things: guideline lag, provider inertia, and patient messaging that stopped at “take your statin.” Most primary care physicians trained when statins were the only game with outcome data, and guidelines take years to catch up with trial results. The cost narrative reinforced it, because PCSK9 inhibitors really were unaffordable in 2015. The evidence covered above tells a different story: three non-statin drug classes now have independent cardiovascular outcome data, costs have dropped dramatically, and one class was specifically designed for statin-intolerant patients. The toolkit changed. The conversation didn’t.
The Verdict: Statin intolerance is a real problem, but “nothing else works” hasn’t been true for years. The toolkit expanded while the narrative stayed frozen.
One Thing I Changed
For the past couple of years, Zetia plus psyllium husk did the heavy lifting. My ApoB went from a peak of 103 to 83 on that combination, without a statin in the picture. Recently I added Repatha, a PCSK9 inhibitor. Early days. I’m watching the numbers settle before deciding what the long-term regimen looks like.
The pattern across the full three-post arc is simple. Stopping one tool is not the same as stopping the work. The toolkit is bigger than most doctors will tell you, and the decisions are granular.
Ask about the full toolkit
If you stopped a statin or can’t tolerate one, the conversation shouldn’t end there. Ask your doctor about ezetimibe, bempedoic acid, or a PCSK9 inhibitor. For my South Asian patients, I start the non-statin conversation earlier than the guidelines technically require, because the risk window is narrower. If cost is a concern, ask about Repatha’s $239/month direct-to-patient program or co-pay cards. Stopping one medication leaves the goal intact: the goal is LDL lowering, and the medication is one tool among several. The tools exist, they’re not exotic, and you have to ask for them by name.
- Dr. Karan Bhalla
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.