
The Best Training Week Is the One You Repeat
Two strength sessions, a little cardio, and a daily walk: the minimum that gets you most of the benefit, what to add, and what changes after 40.


Most people put their energy into the wrong part of exercise. They either spend too much time getting the programming perfectly nailed down, or go all-in on intensity in short spurts, only to fall off the wagon a few weeks later. Far too often, people sign up for the gym as a New Year’s resolution and cancel a month later.
Spoiler alert: the part that has the biggest impact is consistency, and how the week is spaced. The metabolic benefit of a single workout, the improvement in how your body handles glucose, fades within about 72 hours. Go four or more days without anything and you drift back toward where you started. A consistent routine you follow week after week, without long gaps, beats the cleverest program you follow for a month and quit.
This post is the whole picture in one place. What strength training does, what cardio does, why walking is the floor and not the workout, and how to assemble it into a week you can sustain. We wrote it with Trei Tackett, MSN, FNP, an executive health coach and founder of Pillars Health, a precision medicine company, who programs this for a living and has coached hundreds of people over the years.
Two things are non-negotiable, and you need both: strength and cardio. They do different jobs, and done together they beat either one alone. Combined training is associated with about 40% lower all-cause mortality than strength or cardio by itself (British Journal of Sports Medicine, 2022), and a year-long trial of 406 adults found that splitting time evenly between the two matched a full cardio program for cardiovascular risk while adding the muscle that cardio alone misses (European Heart Journal, 2024; randomized controlled trial, n=406). We’ll take them one at a time, then put the week together.
TL;DR
Strength training is non-negotiable. The mortality benefit maxes out at just 30 to 60 minutes a week, and skeletal muscle handles about 80% of the glucose your body clears after a meal
Cardio is non-negotiable too. Low cardiorespiratory fitness is comparable to smoking as a risk factor for early death, and fitness is the single biggest lever on South Asian insulin resistance
Walking is the floor your training stands on, not the workout itself. 7,000 steps a day and breaking up long sitting both matter on their own, before any workout
Never let three days pass without a session. Consistency and spacing beat any specific program
Your muscles run your metabolism
Of the two, strength is the one people skip, and it carries the most leverage. Strength training is associated with 10 to 17% lower risk of all-cause mortality, cardiovascular disease, cancer, and diabetes, and the benefit maxes out at just 30 to 60 minutes a week (British Journal of Sports Medicine, 2022; meta-analysis, 16 studies, n=263,058). That is less time than most people spend choosing a program.
And the case only gets stronger with age, because muscle doesn’t hold steady on its own. After about 30 we start losing it, roughly 3 to 8% per decade, with the decline accelerating after 60 (Frontiers in Physiology, 2012; quantitative review of skeletal muscle aging). Left unchecked, that’s muscle quietly traded for fat, less strength, and a harder time staying independent in your 70s and 80s. Resistance training is the one reliable way to build muscle and hold onto it. Cardio won’t do it, and neither will diet alone.
Muscle is also far more than structural. We tend to think of it as the stuff that moves the skeleton around, but it’s the largest metabolic organ you have. Skeletal muscle is responsible for roughly 80% of the glucose your body clears from the blood after a meal under the influence of insulin (Journal of Clinical Investigation, 1985; DeFronzo et al., euglycemic clamp study). Not the liver, not fat tissue. Your muscles are the primary place sugar goes, and more muscle means a larger, more responsive sink for it. In a large national sample, every 10% increase in relative muscle mass was associated with an 11% lower measure of insulin resistance and a 12% lower rate of pre- or overt diabetes, even after accounting for overall obesity (Journal of Clinical Endocrinology & Metabolism, 2011; Srikanthan and Karlamangla, NHANES III, n=13,644).
This is where South Asians start at a disadvantage. At the same body fat, South Asian men carry about 3.5 kg less lean mass than European men (Journal of Clinical Endocrinology & Metabolism, 2009; Lear et al., n=828). A UK Biobank imaging study found the gap holds even when you match people for sex, age, height, and weight: South Asians had less muscle and more fat, and more than twice the rate of poor muscle composition, 19.9% versus 7.9% (eBioMedicine, 2025; UK Biobank imaging cohort). The “thin-fat” pattern, low muscle paired with high visceral fat, is common in South Asians, and one South Indian cohort put the odds of type 2 diabetes at close to 2.7 times higher even at a normal weight (PLOS One, 2020; Kerala Diabetes Prevention Program baseline, n=1,147). The scale can look fine while the body composition underneath it isn’t.
The good news is that muscle is built the same way in everyone, and it doesn’t take much equipment or time.
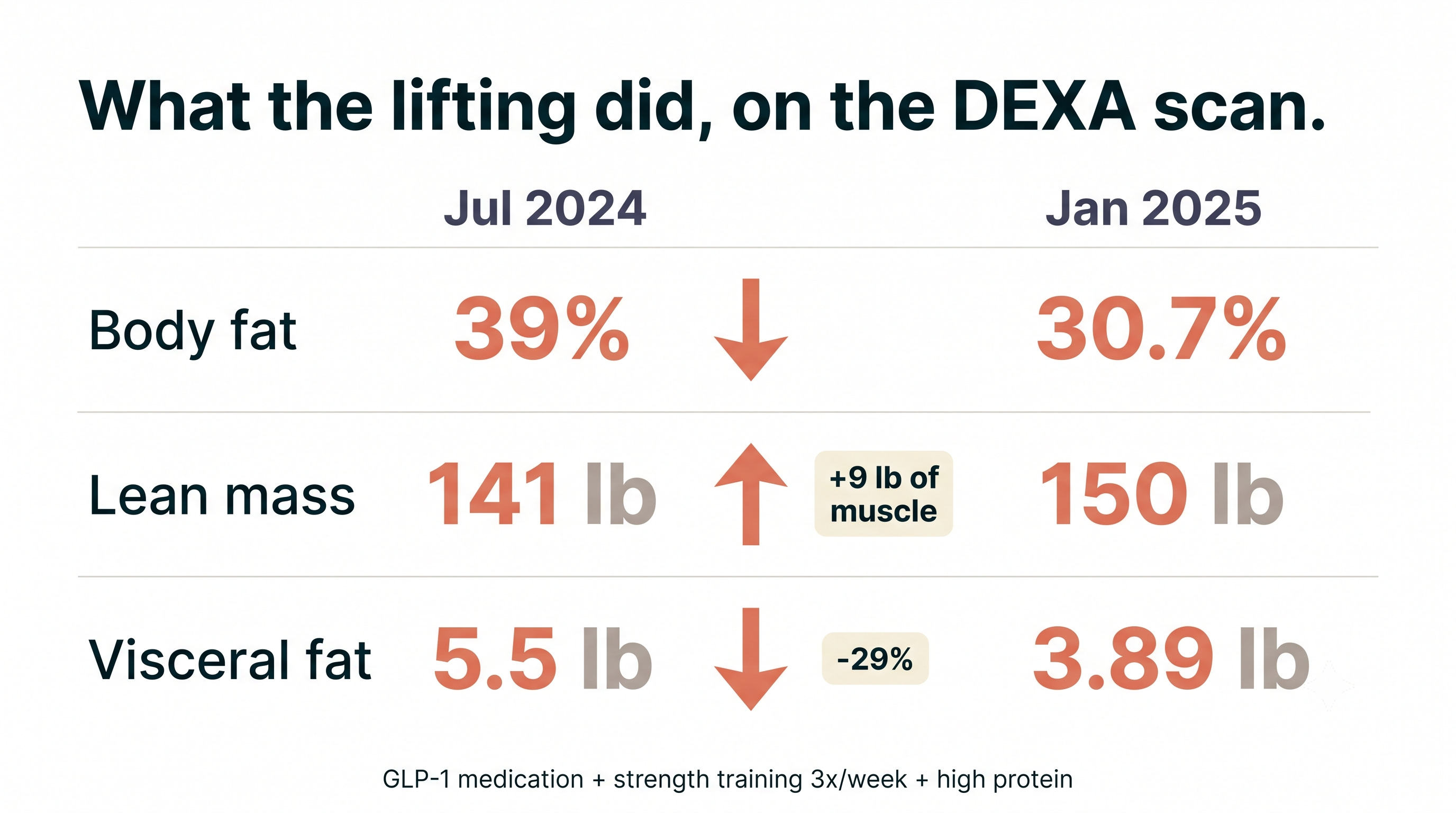
From Amandeep: Between July 2024 and January 2025, my DEXA scans showed something I had to read twice. My body fat dropped from 39% to 30.7%, but my lean mass went up, from 141 to 150 pounds. I gained 9 pounds of muscle while losing fat. Visceral fat fell from 5.5 to 3.89 pounds, a 29% drop. The combination that drove it: a GLP-1 medication, strength training three times a week, and high protein. The lifting was what turned weight loss into the right kind of weight loss.
That last point matters more than ever now that so many people are on GLP-1 drugs like tirzepatide (Mounjaro, Zepbound) and semaglutide. These drugs work, but what you lose depends on what you do alongside them. In the SURMOUNT-1 body-composition substudy, tirzepatide produced 21% weight loss, of which roughly a quarter was lean mass, not fat (Diabetes, Obesity and Metabolism, 2025; n=160 with DXA). For South Asians, who start with less muscle, losing a quarter of it is a worse trade than it sounds.
It doesn’t have to go that way. In a randomized trial, adding a structured exercise program to GLP-1 therapy roughly doubled fat loss while preserving lean mass, compared with the medication alone (New England Journal of Medicine, 2021; Lundgren et al., randomized controlled trial, n=195). Training is what shifts more of the weight you lose toward fat and away from muscle. The minimum worth holding to on these medications: lift at least twice a week, and aim for 1.2 to 1.6 grams of protein per kilogram of body weight per day.
How much strength training is enough, and what kind? Less than you’d guess, and simpler than the internet makes it. The American College of Sports Medicine published its first resistance-training update in 17 years, pulling together 137 reviews and more than 30,000 participants (Medicine & Science in Sports & Exercise, 2026). The headline: the biggest jump comes from going from no resistance training to any. From there, a few things reliably drive strength: lifting heavier loads (around 80% of your one-rep max, heavy enough that the last couple of reps are genuinely hard), through a full range of motion, two to three sets, at least twice a week, done early in the session when you’re fresh. What surprisingly didn’t move the needle: training every set to failure, the type of equipment, how complex the exercises were, or any elaborate periodization scheme. Bands, bodyweight, and home routines all count. You do not need a barbell. You just need to keep showing up.
Cardio is where fitness is won
Where strength protects your muscle and metabolism, cardio protects your heart and your staying power. In a study of 122,007 patients followed for 8.4 years, low cardiorespiratory fitness was comparable to smoking and diabetes as a risk factor for early death (JAMA Network Open, 2018; retrospective cohort). Moving from the low-fitness group to just below average cut mortality risk by about half. Fitness here is VO2 max, how efficiently your body uses oxygen when you push it. You don’t need to measure it to benefit. You need to do cardio regularly.
And fitness isn’t only about living longer. It’s what lets you climb stairs, carry your bags, and keep up on a trip without getting winded at 60 and 70. The more aerobic capacity you build now, the more of it you keep as the years take their cut.
For South Asians, one number reframes the whole conversation. In a comparison of 100 South Asian and 100 European men matched for BMI and age, lower cardiorespiratory fitness explained 68% of the excess insulin resistance in the South Asian group (Diabetologia, 2013; Ghouri et al., n=186). Fitness here isn’t separate from muscle. It reflects how well your muscles and their mitochondria burn fuel, and you raise it by moving more. But the same researchers found something we can’t easily train our way around: South Asian men were less fit than Europeans at every level of physical activity, not because they moved less. The gap appears built into how the muscle handles fuel, which means we may need to train more than the standard guidelines assume to land in the same place. For us, that makes fitness the single highest-return thing to train.
Cardio comes in two gears, and you want both. The easy gear is what’s usually called Zone 2: a conversational pace you could keep up for an hour, breathing a little harder but still able to talk in full sentences. It builds your aerobic base, trains your muscles to burn fat, and costs little to recover from, which is why it should be the bulk of your weekly cardio.
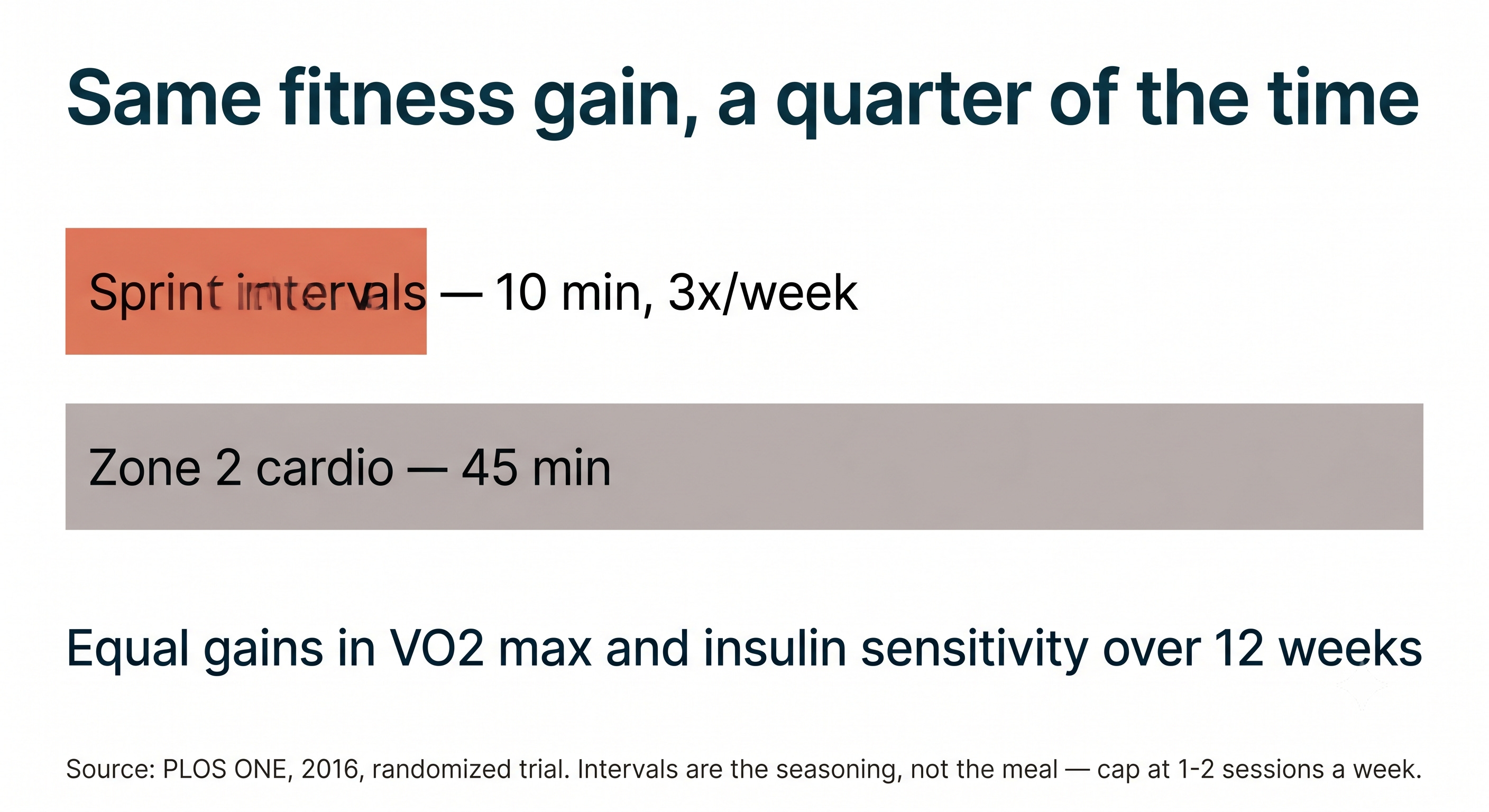
The hard gear is intervals: short bursts of near-maximal effort with easy recovery between them. They raise fitness faster per minute than anything else you can do. In a 12-week trial, 10 minutes of sprint intervals done three times a week produced the same gains in fitness and insulin sensitivity as 45 minutes of Zone 2 cardio (PLOS ONE, 2016; randomized controlled trial). That efficiency is real, but intervals are the seasoning, not the meal. A little goes a long way, and more is not better.
You don’t need a special name or machine. A few interval protocols have the deepest evidence behind them, and the honest truth is that the one you’ll repeat beats the one that’s theoretically optimal.
The Norwegian 4x4, the most studied of them: four rounds of four minutes hard with three minutes easy between, about 30 minutes total.
Sprint intervals, the highest return per minute: three 20-second all-out efforts with two minutes of easy recovery, roughly 10 minutes total.
Tabata, tighter and genuinely hard: 20 seconds hard, 10 seconds easy, eight rounds, four minutes.
Run hills, ride a bike, row, swim, jump rope. The modality matters less than picking something you’ll come back to next week.
If you think high intensity is risky for regular people, the data says otherwise. In supervised programs for patients who already had cardiovascular disease, there was one major cardiac event for every 17,083 sessions (Journal of the American Heart Association, 2018; systematic review). If it’s safe enough for people with heart disease under supervision, most of us can ease into it.
The mistake people make is doing too much of it. Intervals are the most taxing thing per minute that you can do, and more is not better. A small 2025 trial found that two HIIT sessions a week produced the same cardiovascular benefit as three (Physiological Reports, 2025; randomized controlled trial, n=26). Past two or three sessions, recovery cost climbs, cortisol stays elevated, sleep can suffer, and chronically high cortisol can add visceral fat, the opposite of the point. One interval session a week is a great start. Two is the sweet spot for most people.
Intervals also hit two things South Asians tend to carry more of. Running-based interval training reduces visceral fat, the kind packed around the organs, and a review of 19 studies found it cut liver fat by about 2.85%, in less time than Zone 2 cardio takes to do the same (Journal of Clinical Endocrinology & Metabolism, 2022; meta-analysis, n=745). Fatty liver affects roughly a third of South Asians, so that is not a small side benefit.
There’s a reason intervals stick as a habit once you start. Hard efforts trigger a surge in BDNF, the brain protein most tied to focus and learning, along with norepinephrine and endorphins. The heart benefits are the reason to do it. The clear-headed, slightly wired feeling afterward is the reason you’ll want to.
Walking is the floor, not the workout
Walking is baseline movement, the floor that your training stands on top of. It’s how a body is supposed to move through a day, and it sits underneath everything else you do. It’s essential, but it’s movement, not training: it doesn’t load your muscles or tax your heart the way strength and cardio do.
The largest analysis to date found that 7,000 steps a day was associated with 47% lower all-cause mortality, along with lower rates of heart disease, diabetes, dementia, and depression (Lancet Public Health, 2025; meta-analysis, 57 studies). Even 4,000 steps clearly beat 2,000. This is the base your training week stands on, not a substitute for it.
And sitting all day, then doing an hour in the gym, doesn’t undo the sitting. Two-minute walking breaks every 20 minutes during long stretches of sitting cut the glucose response to a meal by 24%, whether or not you also exercised that day (Diabetes Care, 2012; n=19). Prolonged sitting is its own risk factor, separate from how much you train.
One specific habit is worth building, and a lot of our families already have a version of it: a 10 to 15 minute walk after meals. The after-dinner stroll that so many South Asian households grew up with turns out to be better timed than it looks. A review found that walking after eating blunted glucose spikes more than walking before eating, which had almost no effect on the post-meal rise (Sports Medicine, 2023; systematic review). If you wear a continuous glucose monitor, you can watch it happen in real time. The timing is the trick: after the meal, not before.
What a week looks like
Put it together and the picture is simpler than the fitness industry makes it sound.
The minimum that gets you most of the benefit is about two and a half hours a week: two strength sessions of 30 minutes hitting the major muscle groups, one Zone 2 cardio session of 30 to 60 minutes, and 7,000 or more steps on most days. The jump from doing nothing to doing this is the single biggest improvement you can make. Everything beyond it has smaller returns.
When you’re ready to add, here’s the order. A third strength day. More Zone 2 cardio: build toward about 150 minutes a week, spread across two or three sessions, because one session a week barely holds your fitness in place while two or three is where it actually climbs. Then a single interval workout in place of one of those Zone 2 sessions. Ten or fifteen minutes of mobility work after your lifts. Keep intervals capped at one or two sessions a week, because they cost the most to recover from.
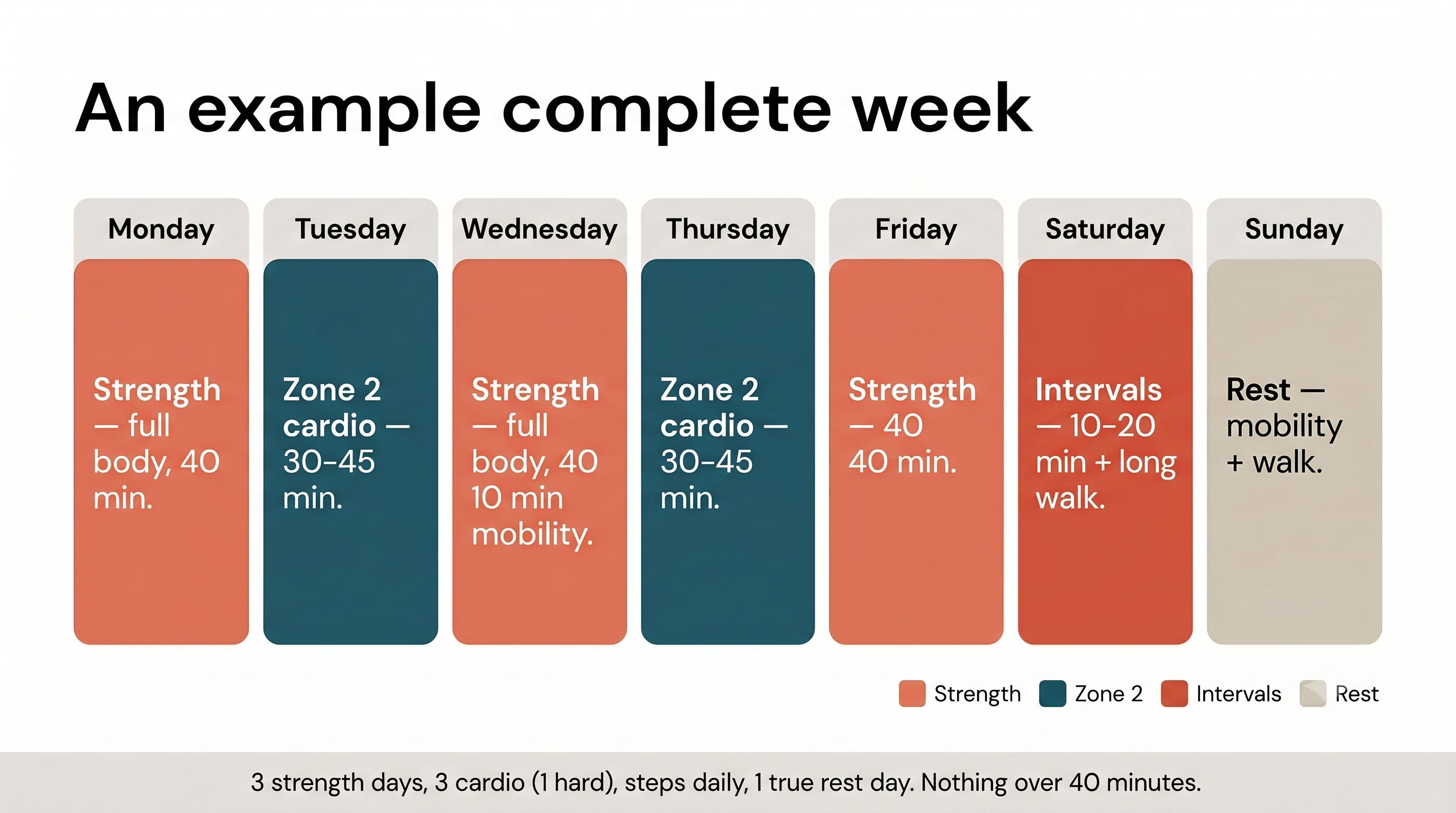
Here’s one way a fuller week can come together:
Monday: strength, full body, 40 minutes
Tuesday: Zone 2 cardio, 30 to 45 minutes
Wednesday: strength, full body, 40 minutes, then 10 minutes of mobility work
Thursday: Zone 2 cardio, 30 to 45 minutes
Friday: strength, 40 minutes
Saturday: one interval session, 10 to 20 minutes, plus the longest walk of the week
Sunday: rest, some mobility, and a walk
That’s three strength days, three cardio sessions with only one of them intense, steps every day, and Sunday as a true rest day. The one tweak Trei makes for most clients is exactly that Thursday slot: a second Zone 2 session, which nudges your weekly aerobic volume toward the 150-minute mark without adding another hard day. Nothing in the week asks for more than 40 minutes at a stretch, and no two days lean on the same muscle groups back to back.
The one principle that runs through all of it: your right amount depends on everything else going on. Someone eating in a deficit and lifting heavy should lean toward Zone 2 over intervals, because the recovery budget is already spent. Stress, sleep, and life load all factor in. The best week is the one you can repeat when work gets busy, not the one that looks best on paper.
Habits > Perfection
The mistake I see most often is people chasing perfection before they’ve created the habit. They start with five days, miss a single day or week due to travel, and quit training for weeks to months. If you’re starting from scratch, pick two days you can protect no matter what, put a full-body strength session on each, and add a 20-minute walk most days. For my clients, I really encourage them to find a time each day that a 20-minute walk makes the most sense. For some, it’s in the morning before the day gets started. For others, walking after lunch keeps energy levels from dropping in the early afternoon. That’s it for the first month. Once those two days are automatic, we add a third session and a little cardio. Build the habit first, then build the program on top of it.
- Trei Tackett
After 40, recovery earns its place
Two things change as you get older, and neither is what most people fear.
The first is recovery. Training status matters more than age: a well-trained 50-year-old recovers faster than an untrained 30-year-old. But the spacing does matter. Leave 48 to 72 hours between hard sessions for the same muscle groups, and treat that gap as part of the program, not a break from it.
The second is mobility and balance, and this is the part that’s easy to skip because the payoff is decades out. Falls are what take people out of independent life in their 70s and 80s. Hip mobility, shoulder range, single-leg balance: the work that prevents that starts now, not at 65. Ten or fifteen minutes after a strength session is enough to start.
What doesn’t change with age is the value of intensity, and that’s the reason not to drift into easy-only training. In a Mayo Clinic trial, 12 weeks of interval training raised mitochondrial capacity by 69% in adults aged 65 to 80, and reversed some of the age-related decline in how muscle builds protein (Cell Metabolism, 2017; randomized trial, n=72). The younger group in the same study gained less. Used in the right dose, hard effort is one of the few things that pushes back on cellular aging, which is exactly why it belongs in the week at 50 and 60, not just at 30.
All of this adds up to one thing that matters more every year: staying injury-free. An injury is the fastest way to break the consistency the whole program depends on, and a tweak you’d have shrugged off at 30 can cost you weeks at 55. The protection is built into the week itself: strength, mobility, and recovery each guard against injury, which is reason enough to keep all three. Beyond that, don’t overtrain, and listen to your body. A nagging ache that won’t settle is information and your body is telling you to back off, let it heal, but keep moving as long as there’s no pain. The goal was never the hardest week. It’s all about consistency and long term compounding.
Where to start this week
We asked Trei to put together a starting routine for someone beginning from scratch. It’s one full-body session, and you do the whole thing on each of your strength days. It needs nothing but your bodyweight or a set of resistance bands. Move through all four exercises in order, resting 60 to 90 seconds between sets, at a controlled tempo: about two seconds to lower, a brief pause, and one to two seconds to lift. The last two or three reps of each set should feel challenging, but never so hard that your form breaks down.
Push (chest, shoulders, triceps): Push-up or dumbbell press, 3 sets of 10. Keep your body in a straight line from head to heels and your core braced. Lower until your elbows reach about 90 degrees, then press back up. If a floor push-up is too hard, elevate your hands on a counter or bench to reduce the load.
Pull (upper back, biceps, rear shoulders): Resistance band row or dumbbell row, 3 sets of 10. Anchor the band at chest height or hinge forward with a dumbbell. Pull your elbows back and down, squeezing your shoulder blades together at the end of each rep. Don’t shrug your shoulders toward your ears.
Hip hinge (hamstrings, glutes, lower back): Romanian deadlift or hip bridge, 3 sets of 10. For the deadlift, push your hips back with a soft bend in the knees and a flat back, lowering until you feel a gentle stretch in the hamstrings. For the bridge, drive through your heels and squeeze your glutes at the top without arching your lower back.
Squat or lunge (quads, glutes, core): Goblet squat or split squat, 3 sets of 10. Hold a weight at your chest and sit back and down, heels planted and chest tall. For the split squat, finish all 10 reps on one leg before switching, lowering your back knee toward the floor under control.
Progression: Once you can finish all three sets of 10 with clean form and two or more reps left in the tank, make it harder by adding resistance, slowing the tempo, or adding a fourth set. Build gradually, not all at once.
Trei’s recommendation: Put those two days on the calendar like a standing meeting, same days, same time. Don’t rely on motivation or willpower. It’s much more reliable to build systems. The clients who succeed long-term aren’t the most disciplined. They make training a default instead of a daily decision. James Clear’s Atomic Habits gives the test for a habit that holds: make it obvious, attractive, easy, and satisfying. Obvious = scheduled. Attractive = keep it light, don’t crush yourself. Easy = a simple plan, movements you’re familiar with. Satisfying = enjoy the mood boost, or a small reward from the smoothie bar when you’re done.
If you take one thing from all of this, it’s that consistency beats optimization, every time. Build the week you can actually repeat, and protect the spacing so three days never pass without a session.
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.