
What to Actually Test and Why
You can't manage what you don't measure. Here's where to start.


In our first post, we looked at why South Asians get heart disease a decade earlier than other populations, and why lifestyle alone doesn’t explain it. The natural next question is: what do you actually do about it?
It starts with knowing your numbers. Not the ones from a standard annual physical, which checks almost none of the markers that matter most for South Asians, but the right ones that help you establish a baseline and track what’s actually happening over time.
In this post, we go through the markers that matter, why they’re important, and how often to check them. The goal is to give you enough context to have an informed conversation with your doctor and to start building your own picture of your cardiometabolic health.
This is not medical advice. It’s what we think is worth testing, why each marker matters, and what we’ve learned from the data.
The blood work your annual physical skips
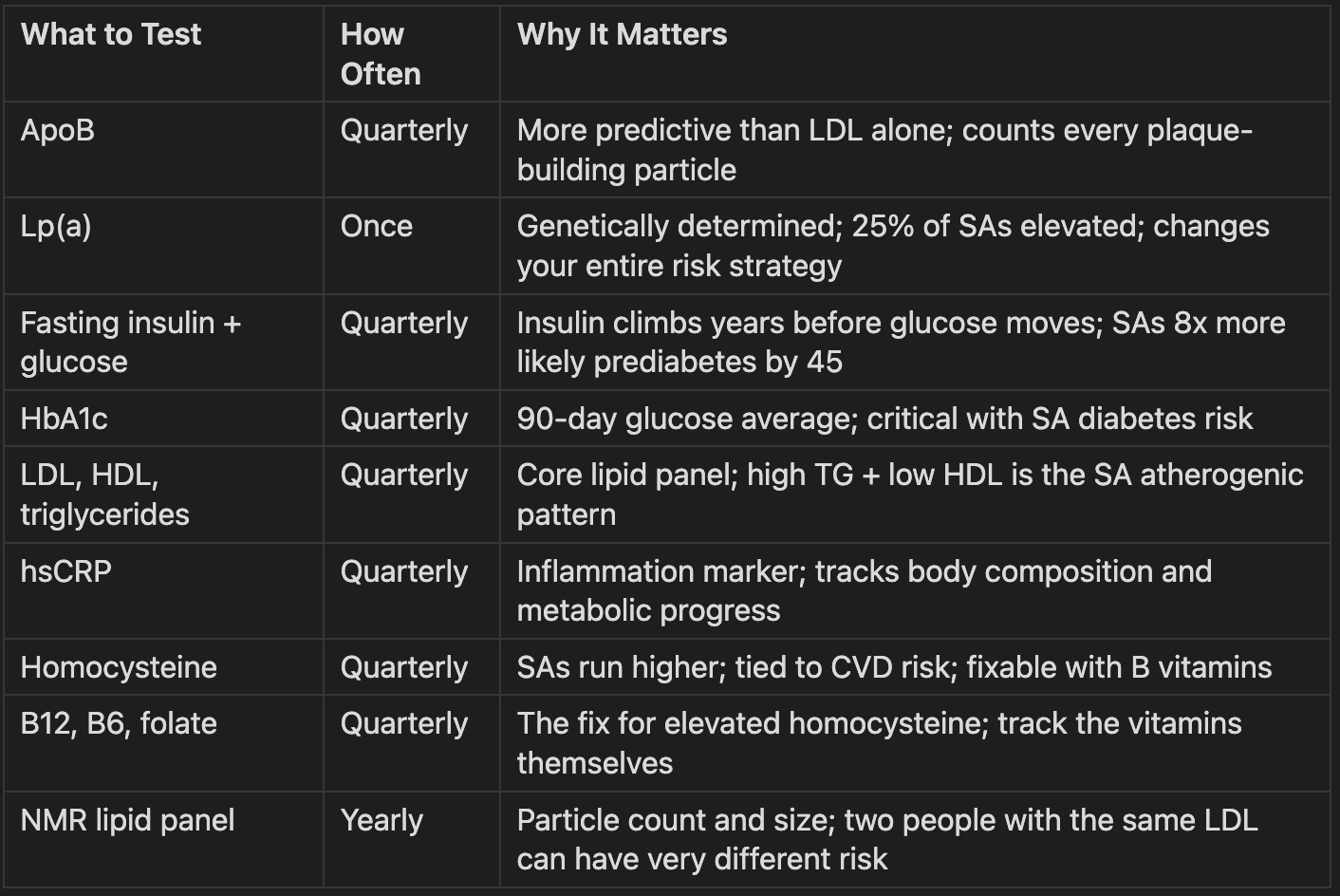
ApoB is the single most important lipid marker most doctors don’t order. It counts every atherogenic (plaque-building) particle in your blood. LDL cholesterol estimates how much cholesterol those particles carry, but ApoB tells you how many particles there are. Two people with the same LDL-C can have very different ApoB numbers and very different risk profiles. If we could only pick one lipid marker, it would be this one.
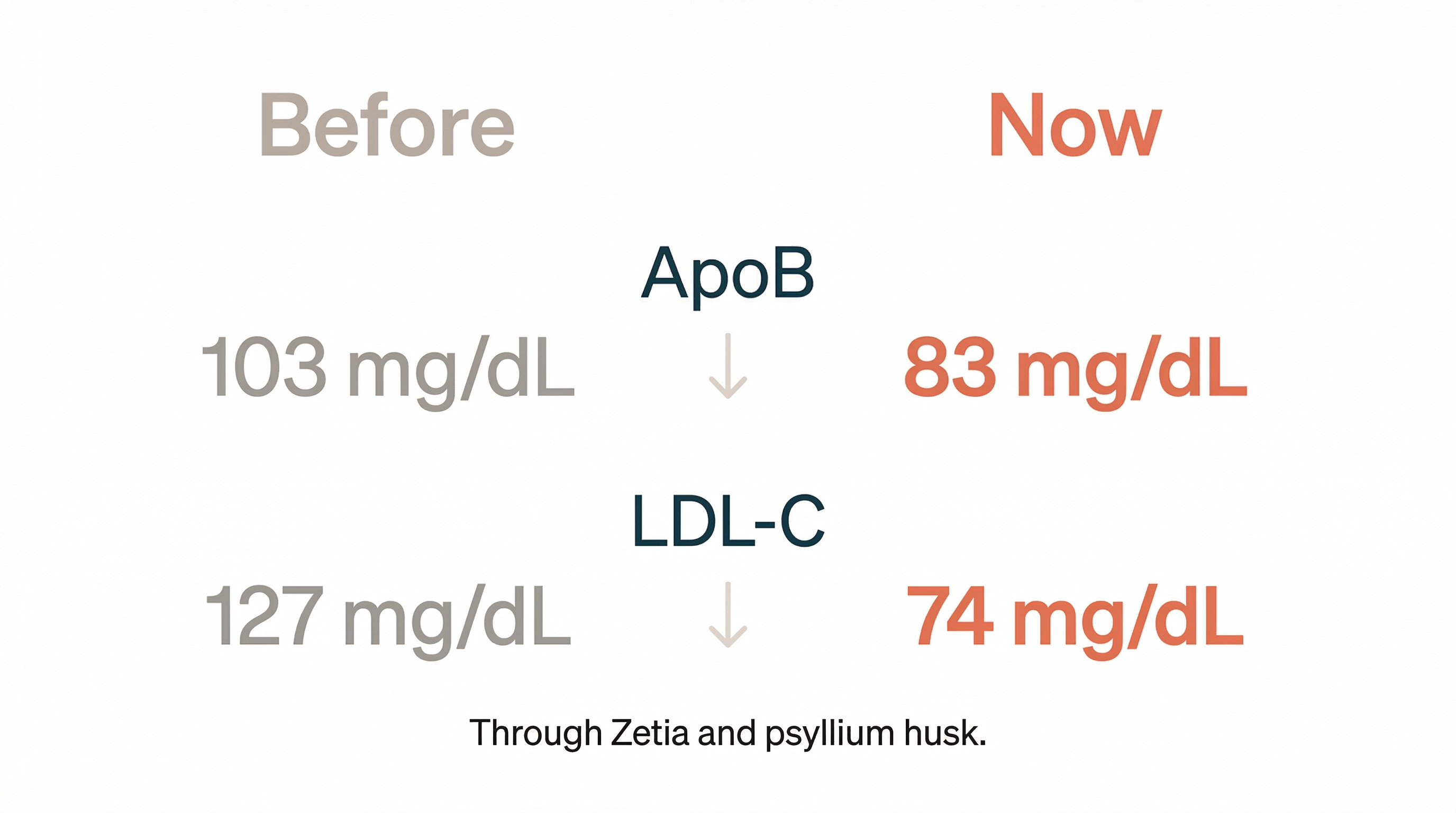
“My ApoB came back at 103 mg/dL. My LDL-C at the time was 127 mg/dL, a number most doctors wouldn’t lose sleep over. A standard lipid panel would never have flagged the problem. Through Zetia and psyllium husk, my ApoB is now 83 mg/dL and my LDL-C is 74 mg/dL. Nobody would have caught it if I hadn’t asked.” -Amandeep
Lp(a) is a genetically determined cholesterol particle that you test once. You can’t diet or exercise it down. 25% of South Asians have elevated levels, and it accounts for 9.5% of heart attack risk in South Asians vs. about 4% in White populations (Circulation, 2019; INTERHEART Lp(a) sub-analysis, n=6,086). If your Lp(a) is high, it doesn’t mean you’re doomed. It means you manage everything else harder: ApoB, blood pressure, glucose. Knowing the number changes the strategy.
Fasting insulin is the one most doctors skip entirely. They’ll order fasting glucose, which is a snapshot of your blood sugar at one moment in time. The problem is that glucose can look normal for years while insulin climbs to compensate. By the time glucose is elevated, insulin resistance has been building for a while. Ask for both fasting glucose and fasting insulin every time. For South Asians, where prediabetes shows up nearly 8x more often by age 45 than in White peers (JAHA, 2026; MASALA/MESA, n=2,700), catching insulin resistance early is the difference between prevention and treatment.
HbA1c is a 90-day blood sugar average that smooths out the day-to-day noise. A single fasting glucose can be thrown off by what you ate the night before. HbA1c gives you the bigger picture. If you have a family history of Type 2 diabetes, this is the trend line that matters most quarter to quarter.
The full lipid panel (LDL, HDL, triglycerides) is where most doctors stop. For South Asians, the pattern to watch is high triglycerides combined with low HDL and small dense LDL particles, what cardiologists call atherogenic dyslipidemia. North Indians develop coronary artery disease at total cholesterol around 170 mg/dL (Indian Journal of Medical Research, 2007), a number most doctors would call normal. Triglycerides are also a useful cross-check against metabolic health: if they’re elevated, something is off with insulin signaling, regardless of what your glucose says.
hsCRP (high-sensitivity C-reactive protein) is a general inflammation marker. Inflammation is one of the drivers of atherosclerosis, and visceral fat is a common culprit. hsCRP moves with body composition: as visceral fat comes down, hsCRP tends to follow. It’s a signal that connects metabolic health to cardiovascular risk.
Homocysteine is an amino acid linked to cardiovascular risk and B vitamin metabolism. South Asians tend to run higher, partly due to higher prevalence of MTHFR variants and partly due to vegetarian diets that are low in B12. The fix is usually B vitamins, which is why we recommend also tracking B12, B6, and folate to make sure you’re actually replete. Elevated homocysteine is common and fixable, but you have to know it’s there.
Advanced lipid panel (NMR) is worth getting once a year. It breaks down particle count and size: LDL-P, small dense LDL, HDL particle number. Two people with the same LDL cholesterol can have very different risk profiles depending on how many particles they have and how big they are. That said, the markers that actually get treated are LDL and ApoB. If those are in a good place, the doctor isn’t going to treat the particle sub-fractions independently. The NMR gives context, but ApoB is where the clinical decisions happen.
The imaging that blood work can’t replace
Blood work tells you what’s in your bloodstream. Imaging tells you what it’s done to your arteries.
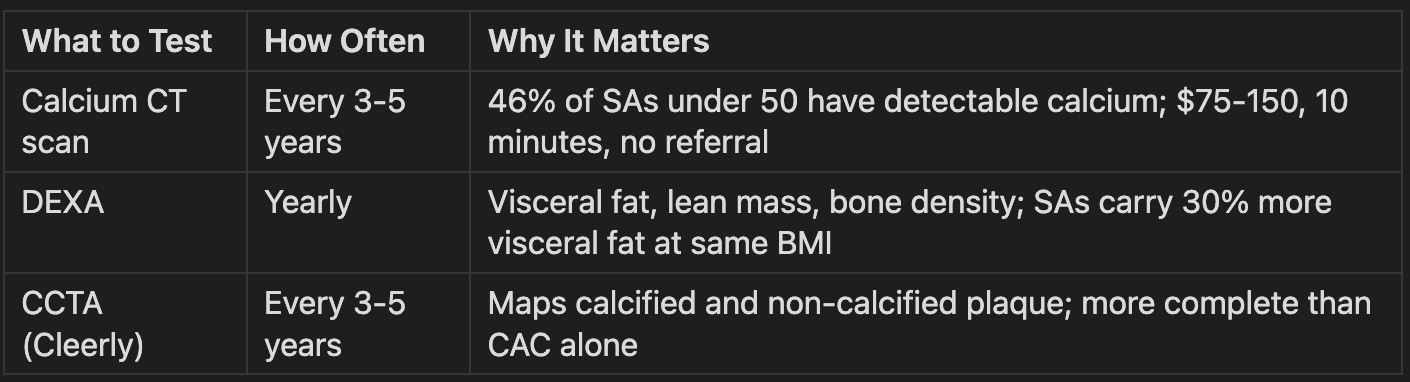
Coronary artery calcium (CAC) scan is a 10-minute CT scan, typically $75-150, and most places don’t require a referral. It measures calcified plaque in your arteries. MASALA data shows that 46% of South Asians under 50 already have detectable calcium (MASALA, PMC9830106). A score of 0 is reassuring. Anything above 0 tells your doctor how aggressive to be with prevention.
A Cleerly CCTA (coronary CT angiography) goes a step further, mapping both calcified and non-calcified plaque. It’s more expensive and involves contrast dye, so it’s not for everyone, but if you have significant family history, it gives a more complete picture than CAC alone.
“My CCTA came back clear: zero plaque burden and a CAC score of 0, despite decades of NAFLD and metabolic dysfunction. Reassuring, but not permanent. I’ll repeat it in 3-5 years.” -Amandeep
DEXA scanning is one of the most underused tools in preventive health. Most people think of it as a bone density test, but a full-body DEXA shows body fat percentage, lean mass, and critically, visceral fat, the metabolically dangerous fat wrapped around your organs that drives inflammation and insulin resistance. A scale tells you your weight changed. A DEXA tells you what changed. At the same BMI, South Asians carry 30% more visceral fat than other populations (International Journal of Obesity, 2016; MASALA/MESA, n=906). The scale won’t catch that. A DEXA will.
Other relevant markers to consider
These aren’t the core cardiometabolic panel, but they each connect to the bigger picture.
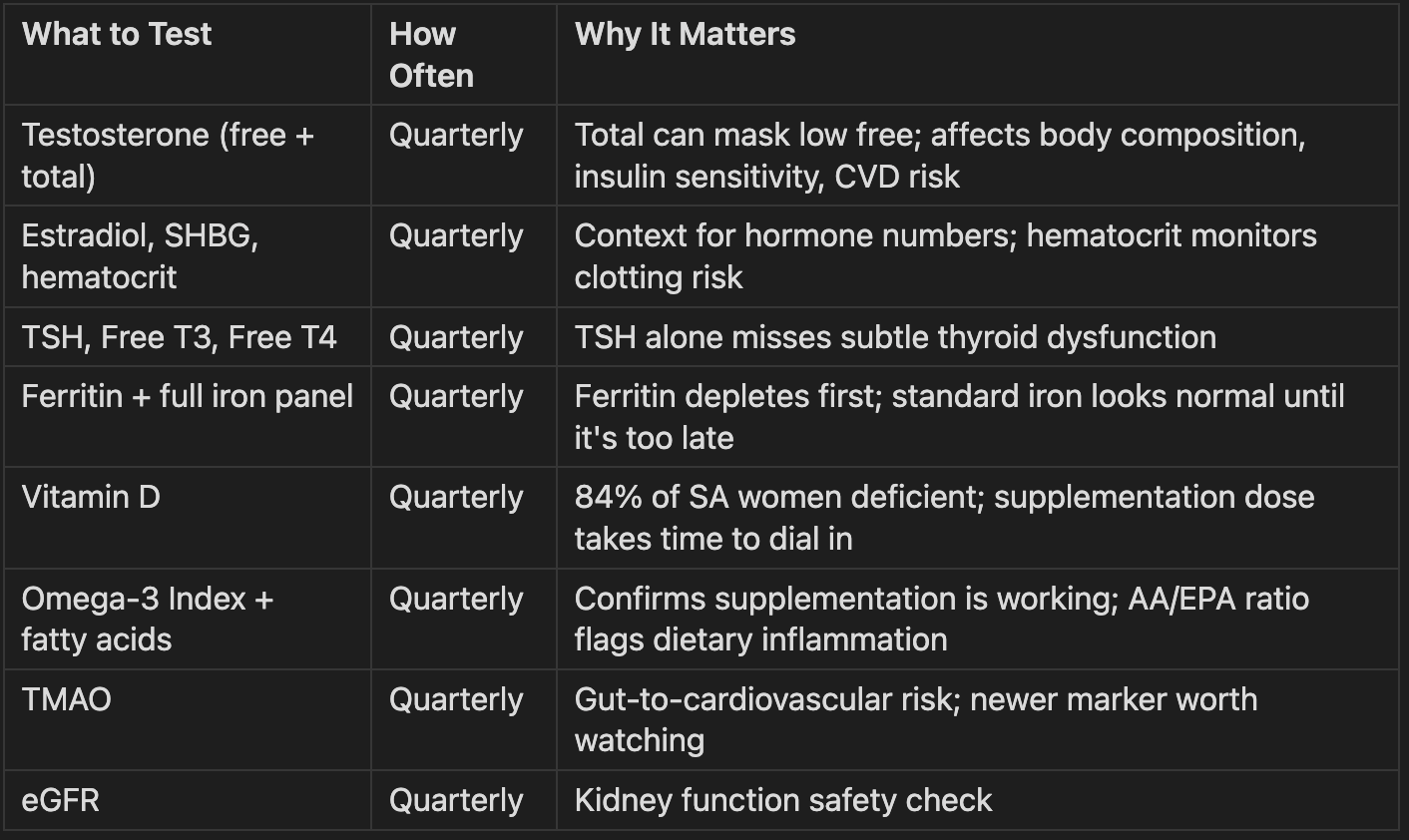
Testosterone (free and total) matters more in your 40s than most men realize. Total testosterone is what most doctors check, but free testosterone is the fraction that’s actually bioavailable. A solid total number can mask low free testosterone. Low T affects body composition, insulin sensitivity, mood, and cardiovascular risk. Ask for both.
Estradiol and SHBG give context to the testosterone numbers. Estrogen matters in men too: too high or too low affects mood, body composition, and cardiovascular risk. SHBG (sex hormone binding globulin) binds testosterone and makes it unavailable, so it’s the context that makes the other hormone numbers make sense.
TSH, Free T3, Free T4 cover thyroid function. Most doctors only order TSH. Free T3 is the active hormone cells actually use, and TSH alone can miss subtle dysfunction. Ask for all three.
Ferritin and full iron panel (iron total, TIBC, transferrin, iron saturation) are important because ferritin depletes first, long before iron total or hemoglobin drop. Without the full panel, depletion doesn’t show up until it hits as fatigue and poor recovery.
Vitamin D deserves a mention because 84% of South Asian women are deficient. Darker skin, indoor lifestyles, and clothing coverage all contribute. Supplementation is common but the right dose varies by individual, so track quarterly until you find it.
Omega-3 Index and fatty acid panel measures whether supplementation is actually working. The target is an Omega-3 Index above 8%. The ratio between omega-6 and omega-3 tells you whether chronic inflammation is being fueled by diet.
TMAO (trimethylamine N-oxide) ties gut microbiome health to cardiovascular risk. It’s a newer marker and not many people track it, but given the cardiovascular focus of this newsletter, it’s worth knowing about.
eGFR is a kidney function check. Kidneys filter everything: supplements, medications, metabolic waste. If kidney function is declining, you want to know early.
What all and how often
Blood work
Imaging
Other markers to consider
How to get started
You don’t have to do all of this at once.
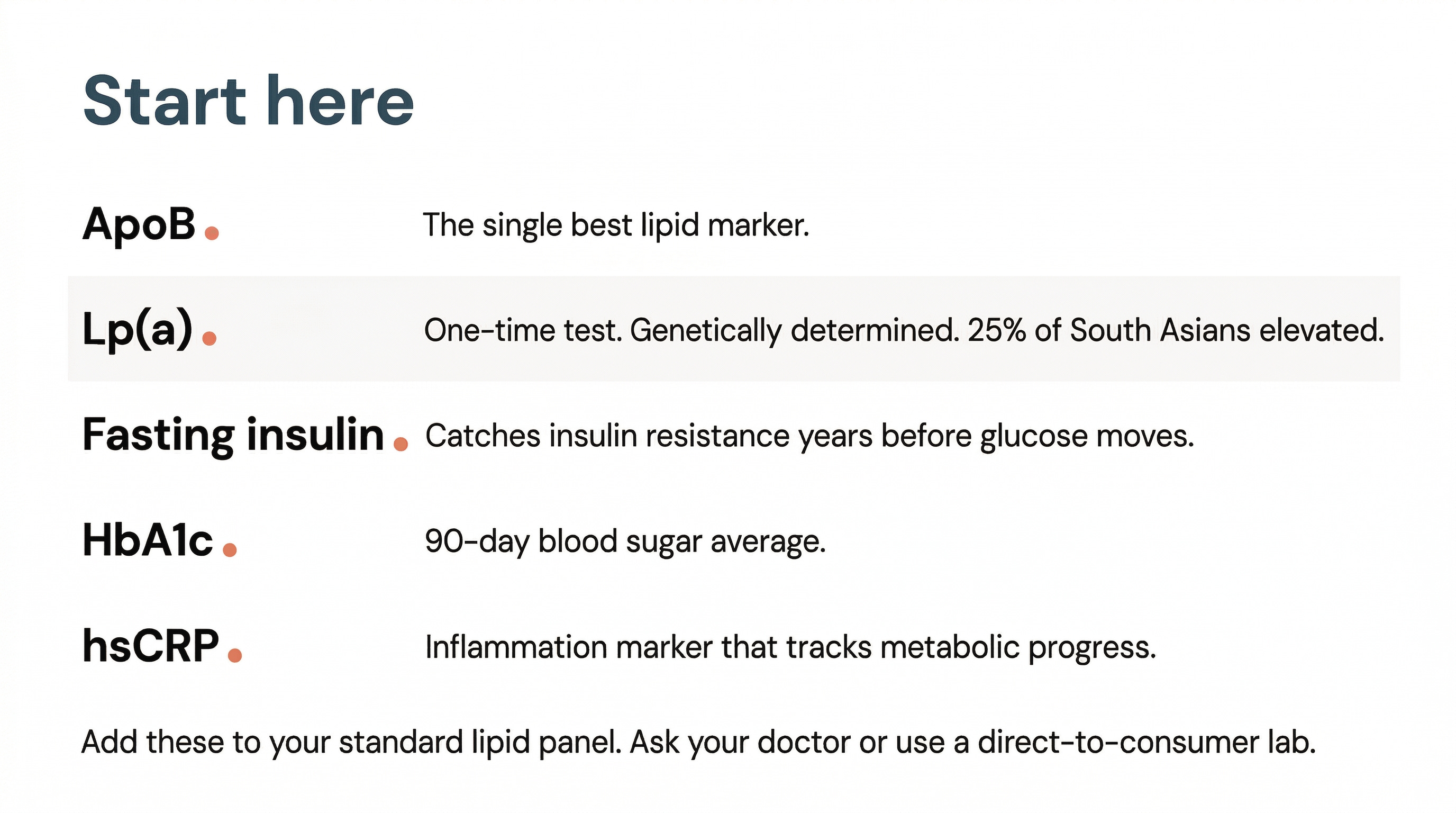
If you’re South Asian and haven’t done anything beyond a standard physical, start here: ApoB, Lp(a) (once), fasting insulin, HbA1c, and hsCRP. These five tests, added to your standard lipid panel, will tell you more about your cardiometabolic risk than most people learn in a decade of annual physicals. Most can be added to a standard blood draw by asking your doctor. If your doctor pushes back, services like Function Health, Marek Health, or a direct-to-consumer lab can run them without a referral.
From there, consider a CAC scan if you have family history or are over 35. Consider a DEXA if you want to know what’s happening under the surface with visceral fat and lean mass.
If you’re actively managing multiple risk factors, quarterly blood work timed with a doctor check-in is ideal. For someone in maintenance mode, twice a year or even annually is enough for most markers. Lp(a) is a one-time test. Calcium CT every 3-5 years. DEXA annually.
The point is to track the right things and establish a longitudinal record of your body so you can catch things in time.
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.