
Why Standard Vitamin D Doses Fail South Asians
The number your lab calls "adequate" was set for bone health. Your metabolism needs more.



This week’s issue is co-authored with Dr. Tiffany Mullen, DO, a functional medicine physician and founder of Vytal Health.
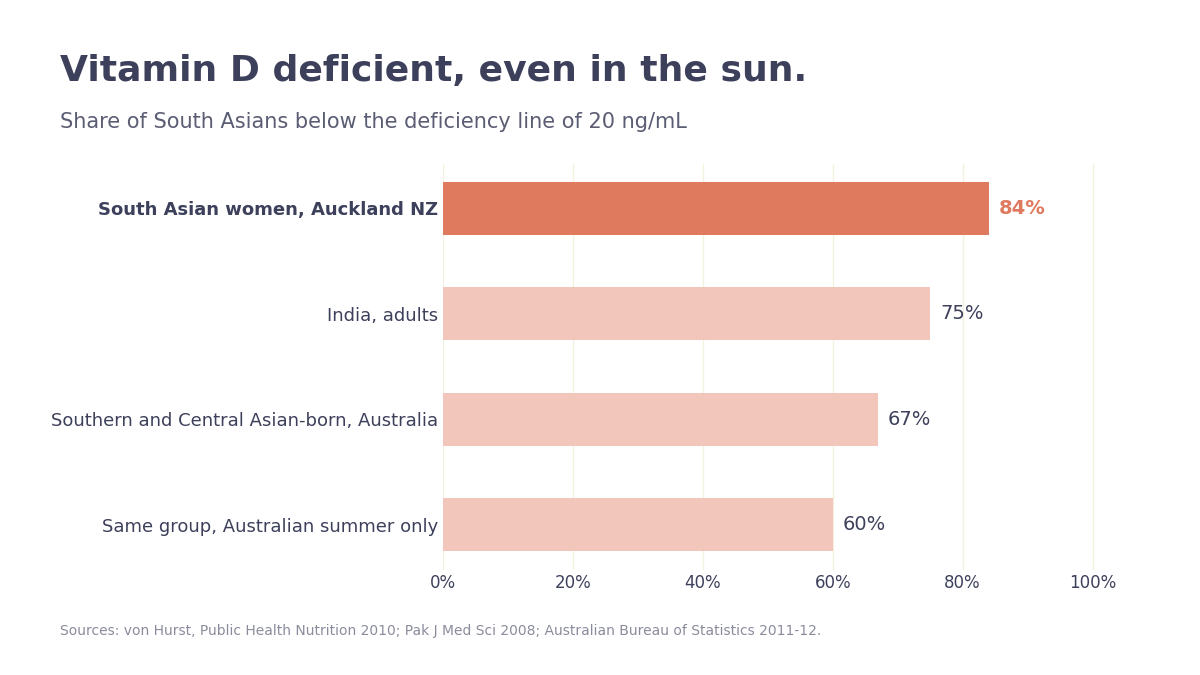
In Auckland, New Zealand, 84% of South Asian women tested below the vitamin D sufficiency line, with a median level of just 11 ng/mL. That is deep deficiency, in a country famous for its sun.
My family in India, one of the sunniest places on earth, runs low too. I live in the Bay Area in California (plenty of sun), and I run low without high dose supplementation. If you are South Asian, this probably sounds familiar - a parent put on vitamin D after a fracture scare, or a doctor who mentioned in passing that people like us are usually deficient. The pattern is common: the people with the most sun overhead were the most deficient inside.
That is the paradox I want to walk through. Because once you understand why it happens, the standard advice your doctor gives you, take 600 to 800 IU and you are covered, stops making sense for people with dark skin.
TL;DR
South Asians are among the most vitamin D deficient people on earth, even in sunny climates: in one Auckland study, 84% of South Asian women fell below the sufficiency line (Public Health Nutrition, 2010; cross-sectional, n=228).
The standard recommendation of 600 to 800 IU a day was built to protect bone in mostly light-skinned populations, and it routinely underdoses South Asians.
In South Asian women, insulin resistance only improved once vitamin D climbed past 32 ng/mL, well above the “adequate” line of 20 (British Journal of Nutrition, 2010; randomized trial, n=81).
Vitamin D is a hormone with both a floor and a ceiling: correcting a real deficiency helps, but chasing very high levels backfired in trials (more falls, less bone), so aim for a range rather than a maximum. South Asians are far more likely to be starting below it.
The sun can’t fix this for us
Start with how strange the data is. In India, Pakistan, and Bangladesh, countries with abundant year-round sun, cohort after cohort puts roughly 70 to 80% of adults below 20 ng/mL, the line where most labs call you deficient (review of South Asian studies, Pakistan Journal of Medical Sciences, 2008). In Australia’s national survey, 67% of people born in Southern and Central Asia were deficient, and 60% stayed deficient even in summer (Australian Bureau of Statistics, 2011-12 National Health Measures Survey).
Five things stack up against us, and they compound.
Skin. Melanin is natural sun protection, so darker skin makes far less vitamin D per minute of sun, several times less than fair skin. (How many minutes that actually costs you is the next section.)
Body fat. Vitamin D is fat-soluble, so it gets pulled into fat tissue and out of circulation. South Asians carry more body fat at a given weight, so more of the vitamin gets stored instead of used, and people with higher body fat often need two to three times the dose to reach the same blood level (Endocrine Society guideline, JCEM, 2011).
Sun avoidance. Indoor work, plus a cultural premium on staying fair, keeps a lot of skin covered, especially for women.
Diet. Few foods carry much vitamin D, and UK South Asians average just 1 to 3 micrograms a day from food, a fraction of what you need (UK Biobank data, Proceedings of the Nutrition Society, 2020).
Genetics. Common variants in the genes that make and carry vitamin D leave some people lower for the same sun and the same dose.
Put them together and casual sun plus a token supplement does not move the needle.
On sun alone, 25 minutes a day, and not in winter
The obvious fix is to just go outside, so it is worth knowing the actual number. For South Asian skin, it takes roughly 25 minutes of midday sun with your forearms and lower legs bare, most days, to hold a healthy level. Fair skin gets there in about 9 minutes (Webb et al., Nutrients, 2018). The melanin that protects you is the same thing that roughly triples the clock.
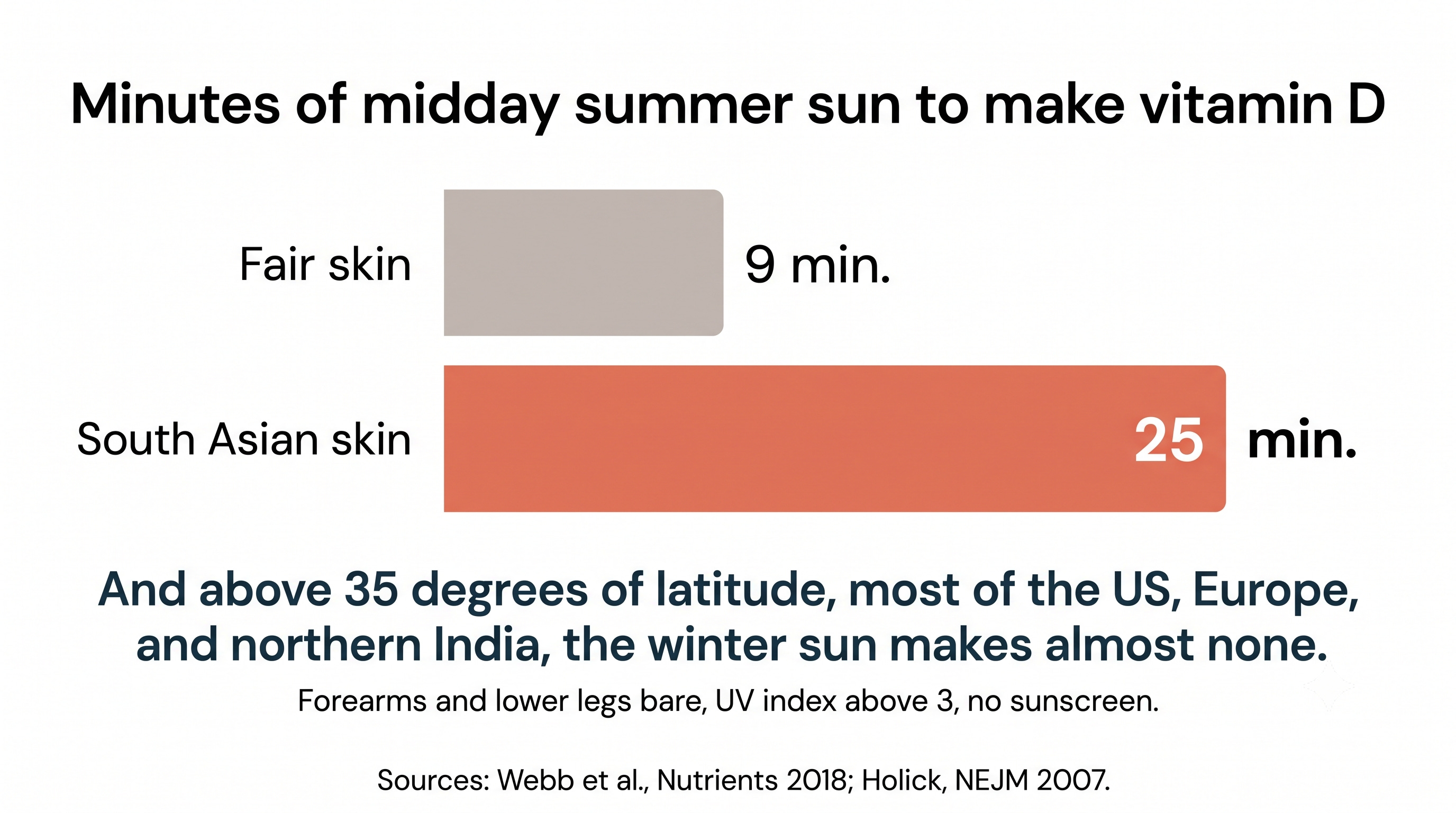
And those minutes only count under real conditions: midday, when the UV index is above 3, with no sunscreen (an SPF of 8 blocks most of the rays you need) and arms and legs actually bare, not just hands and face. Above about 35 degrees of latitude, which covers most of the United States, Europe, and northern India, the winter sun sits too low to make much vitamin D at all, for months at a stretch (Holick, NEJM, 2007). The one piece of good news: you cannot overdose this way, because your skin stops once it has made enough.
So yes, the sun can do it, at midday, in the sunny months, with your limbs bare, for 25 minutes most days. For most of us, most of the year, that is not a plan you can count on. Which is why you supplement to a target instead. The question is what that target should be.
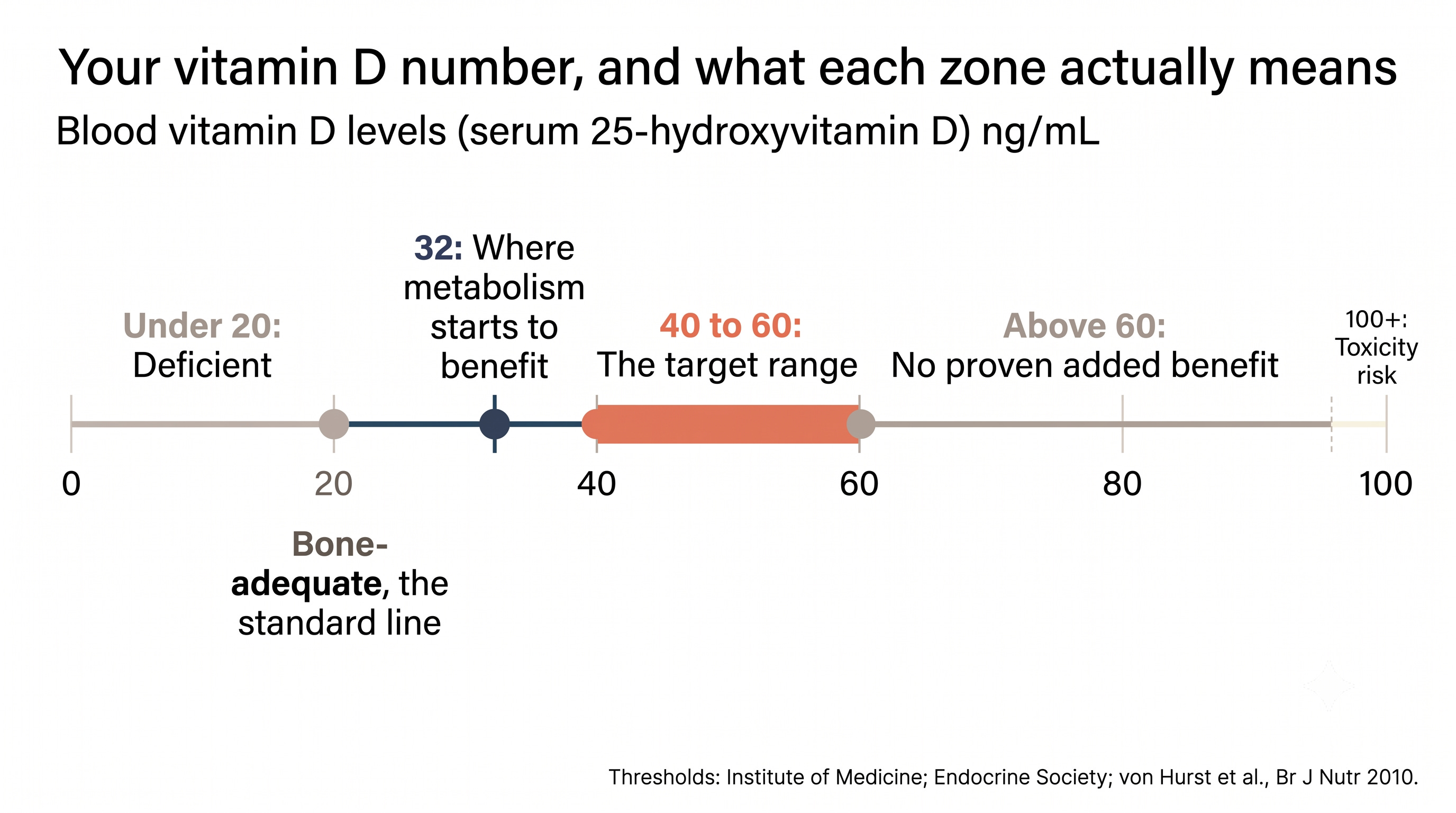
20 is a bone number, not a metabolism number
For anyone watching their metabolic health, the standard target is set too low, and here is why.
The “adequate” line most labs use, 20 ng/mL, comes from the Institute of Medicine. It was set to prevent rickets and protect bone, modeled mostly on light-skinned populations, assuming some sun and decent calcium intake. It was never designed around insulin, diabetes, or heart disease. It answers one question: are your bones covered?
Your metabolism appears to want more. In a randomized trial, 81 insulin-resistant South Asian women in New Zealand took either 4000 IU of vitamin D a day or a placebo for six months. The supplemented group improved their insulin sensitivity and dropped their fasting insulin, but the benefit only showed up once blood levels passed 32 ng/mL, with the best range landing between 32 and 48 (British Journal of Nutrition, 2010; randomized trial, n=81). At 22 ng/mL your lab says “sufficient” and your doctor moves on. Your bones may be fine there. The metabolic benefit in these women did not appear until they were ten points higher.
But the big trials look mixed
The trials on this are genuinely mixed, and you should know it. When researchers pooled 18 randomized trials, vitamin D supplementation showed no overall effect on insulin sensitivity (Diabetes Care, 2020; meta-analysis, n=1,220), and the largest diabetes-prevention trial gave 4000 IU a day to people with prediabetes and saw no significant drop in who progressed to diabetes (NEJM, 2019; randomized trial, n=2,423).
So which is it? The two findings reconcile cleanly. Vitamin D behaves like a floor, not a lever. Climb out of deficiency and you may gain something; keep adding once you are already sufficient and nothing much happens. That diabetes-prevention trial never screened for deficiency, so most people started near 28 ng/mL with no floor to climb off, while the South Asian trial enrolled women who were deficient and insulin resistant and pushed them past the threshold. The benefit lives in the climb out, and South Asians, already wired toward insulin resistance at lower body weights, are far more likely to be starting down there. It is the same thread I pulled on in the fasting insulin issue: the standard target is aiming at the wrong number for the wrong population.
Vitamin D is a hormone, and hormones have a ceiling
So your metabolism wants more than the standard target. There is an upper bound too, though, and finding it changed how I think about my own dose. Vitamin D is not really a vitamin. Your body converts it into calcitriol, a steroid hormone from the same family as cortisol and the sex hormones, and it behaves the way hormones do, switching genes on and off and controlling how much calcium moves through your blood. Calling it a vitamin makes it sound like vitamin C, where the excess just leaves in your urine. It does not. It is fat-soluble, it accumulates, and it acts through a receptor.
So the dose has a ceiling, and you can overshoot it. Push your level too high and you get too much calcium in the blood and urine, which can mean kidney stones and, the part that matters for anyone watching their heart, calcium settling into soft tissue like artery walls.
The trials are blunt about this. When more than 2,200 older women were given a single 500,000 IU dose of vitamin D once a year, they had 26% more fractures and more falls than the placebo group, with the spike worst in the first three months (Sanders et al., JAMA, 2010; randomized trial, n=2,256). And when healthy adults took 400, 4,000, or 10,000 IU a day for three years, the higher doses did not build bone, they lost slightly more of it, in a clean dose-response (Burt et al., JAMA, 2019; randomized trial, n=311). In both trials, the higher the dose, the worse the result.
So where is the real ceiling? Higher than the 20 most labs fixate on. The range most functional-medicine clinicians aim for is 40 to 60 ng/mL, where the benefit is best supported and the risk stays low. Above 60, the added benefit is unproven for general health, and the highest-dose arm of that bone trial, the group on 10,000 IU a day whose levels climbed into the 70s, lost the most bone. Frank toxicity, the hypercalcemia kind, is rarer still and shows up far higher, north of 100. None of this is a reason for fear. It is a reason to aim for a range: correct a deficiency, settle into the 40s or 50s, and stop chasing a bigger number.
From Amandeep: I take 5000 IU a day, which is above the 4000 IU daily ceiling most guidelines set for routine use, and I do it on purpose. My genetic panel flagged a variant in my vitamin D receptor, the docking station the active hormone binds to (the gene is called VDR). My conversion genes are normal, so for me the bottleneck is not making or storing vitamin D, it is the receptor reading it. That is part of why the same dose lands two people at completely different blood levels: your genes, your body fat, and your sun exposure all move the result. The science tying a specific receptor variant to a specific dose is still emerging, so I treat it as one input, not a verdict. It nudged my personal target higher, to 45 to 65 ng/mL, and my last test landed at 55 (April 2026), inside the healthy range but on a bigger dose than most people need. Because I run that high a dose, I track my blood calcium (normal so far) and pair the D with vitamin K2 (the MK-7 form), which helps steer calcium toward bone instead of arteries.
Myth: “Brown skin adapted to the sun, so I get plenty of vitamin D”
The Myth: People with South Asian skin evolved under strong sun, so we are naturally good at making vitamin D and do not need to worry about it, especially if we live somewhere warm.
The Evidence: The exact opposite is true, and the mechanism is the giveaway. Melanin protects skin by blocking some of the UVB that triggers vitamin D production, so darker skin makes less per minute of sun, not more. That is why 84% of South Asian women in sunny Auckland tested deficient (Public Health Nutrition, 2010; n=228), and why 60% of Southern and Central Asian-born Australians stayed deficient through summer (ABS, 2011-12). Add indoor lives and clothing that covers arms and legs, and the one advantage, abundant sun, never reaches the skin.
The pigment that protects us from the sun is the same pigment that keeps us from making vitamin D from it. Warm weather does not fix this.
From Amandeep: One Thing I Changed
I stopped treating my vitamin D dose as fixed and started treating it as a dial. I moved my testing to a regular cadence and adjusted the dose against the result, the same way I would tune any other marker. The point was never to hit a big number. It was to land in a range on purpose instead of hoping a standard dose was enough.
Vitamin D is a deficiency worth correcting, especially in a population that is deficient by default and metabolically vulnerable on top of it. That is a modest, well-supported claim, and it is enough.
Test, then target 40 to 60 ng/mL
In functional medicine, we test vitamin D as a matter of routine rather than waiting for a reason, because the only way to know your number is to measure it. Ask for a 25-hydroxy vitamin D test, which is the standard vitamin D blood test your doctor already runs, know your number, and aim for the 40 to 60 ng/mL range rather than just clearing the 20 ng/mL “normal” line. Getting there often takes 2000 to 4000 IU a day, sometimes more if you carry extra weight or the VDR gene variant. Recheck about three months after any dose change, because levels take that long to settle. If you live somewhere with dramatic seasons, as I do in Wisconsin, it helps to test at different times of year to see how much the sun is adding to your supplement in your own blood level. One caution worth naming: newer population guidelines actually advise against routinely testing healthy adults, including those with darker skin. For anyone with darker skin or a strong family history, I think knowing your number is worth the test, so the dose can be personalized.
-Dr. Mullen
Disclaimer: The information provided in this article is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare providers with any questions you may have regarding a medical condition or wellness program. Reliance on any information provided in this article is solely at your own risk. The author and publisher of this article make no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or effectiveness of the information contained herein. The inclusion of specific products, services, or strategies in this article does not imply endorsement or recommendation. The author and publisher disclaim any liability for any adverse effects or consequences resulting from the use or application of the information presented. You are encouraged to consult with a qualified healthcare professional before making any changes to your diet, exercise routine, or lifestyle.
 | A guest post by
|